Updates on nutrition for optimizing preterm growth
Preterm infants have a high risk of malnutrition, poor growth and poor health outcomes. Updated, recommendations for enteral nutrition of preterm infants will be issued from the ESGPHAN. They will cover recommended intakes of macro- and micronutrients as well as evidence-based recommendations on feeding practice and clinical management.
New ESPGHAN guidelines for enteral nutrition: Practical aspects
Abstract
Infants born very preterm or with a very low birth weight have a high risk of malnutrition, poor growth and poor health outcomes. Suboptimal nutrition of preterm infants has been associated with severe metabolic disturbances, sepsis, necrotizing enterocolitis, osteopenia, bronchopulmonary dysplasia, retinopathy of prematurity and poor neurodevelopment.
The field of preterm nutrition is a very active research area and improved nutrition has thus been identified as one of the most important targets for quality improvement within neonatology. In 2010, the European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ESGPHAN) issued guidelines for enteral nutrition of the preterm infant, and these have been extensively used and cited. However, since the evidence base has grown rapidly, it is now time for an update.
The new guidelines, which will be published within the next 6 months, will include not only recommended intakes of all macro- and micronutrients, but also evidence-based recommendations on feeding practice and clinical management. The topics include e.g. initiation and advancement of enteral feeds, measurement of gastric residuals, the transition from parenteral to enteral nutrition, mode of feeding, growth monitoring, use of breast milk and fortification of breast milk, osmolarity and bioactive food supplements.
The guidelines are aimed at stable, growing infants with a birth weight < 1800 grams. They will not cover critically ill infants or post discharge nutrition. Recommended macronutrient intakes will be similar to the previous guidelines, except slightly higher upper limits of intakes. In contrast to the previous guidelines, recommended intakes of a range of long-chain poly-unsaturated fatty acids will be specified. Recommended intakes of potassium, calcium, phosphorus, zinc and copper will be higher than in the previous recommendation. Vitamin D intake will be given per kg per day rather than per day as in the previous recommendation.
Examples of the new recommendations regarding feeding practice and clinical management follow: Small volumes of enteral feeds should be started as soon as possible after birth and feeds should be advanced as clinically tolerated. In stable preterm infants, a routine daily increment of 18-30 ml/kg/day is recommended. Routine monitoring of gastric residuals in clinically stable infants is not recommended. Growth should be monitored regularly, e.g. daily weight measurements and weekly length and head circumference measurements. Fortifcation of human milk using multinutrient fortifers is recommended. Probiotic supplementation is recommended for prevention of necrotizing enterocolitis. Despite some promising early research, other bioactive food supplements are currently not recommended for routine use in preterm infants. Local, standardized protocols for feeding, growth monitoring and management of growth faltering should be implemented.
Human Milk Oligosaccharides and the preterm infant: clinical relevance
Key Message
→ In premature infants, gut microbiota shows diferent patterns related with NICU practices and maturity. It is associated with the level of HMOs in breastmilk. Specifc HMOs milk content may be associated with decreased NEC and LOS. HMO supplementation might reduce dysbiosis leading to more mature microbiota and better clinical outcome.
Abstract
Gut microbiota plays an important role in the health of infants. Breastfed term infants have a gut microbiota that is dominated by bifdobacteria, whereas formula-fed infants have a more heterogeneous composition.1 This prevalence of bifdobacteria has been associated with reduced infection rates and less allergy manifestation as compared with formula-fed infants.1 However, few data are available to support microbiota composition and its impact on premature infants’ health. In a prospective observational cohort study of 577 preterm newborns < 32 weeks gestation, Rozé et al2 classifed gut microbiota with regards to the most abundant bacteria present in the stool sample. Six clusters (Clst) were identifed and respectively driven by Enterobacter (Clst1), Clostridium (Clst2), Escherichia Coli (Clst3), Enterococcus (Clst4), Staphylococcus (Clst5) and a sixth cluster with non-amplifable samples owing to low bacterial load. Perinatal determinants were associated with microbiota: Clst 4-6 were signifcantly associated with lower gestational age and Clst3 with more mature infants. Birth by cesarean delivery was associated with increased risk of having an immature cluster. Conversely, no ventilation on day 1, direct breastfeeding, and skin-to-skin practice were associated with the more mature Clst3. Late onset sepsis occurred signifcantly more often in the most immature clusters which were also signifcantly associated with 2-year non- optimal outcome defied by death and/or neurodevelopmental delay.2 Overall, this study suggests that gut microbiota of very preterm newborns is not dominated by bifdobacteria in early life but may be related to infants’ maturity, perinatal determinants and may be associated with the outcome.
Microbiota may be modulated by pro- or prebiotics. Among the latest, human milk oligosaccharides (HMO) are structurally diverse, indigestible to the infant, thus reaching the lower gastrointestinal tract intact where they may act as substrates for bacteria such as bifdobacteria.3 They also have antimicrobial and immune properties, consequently reducing allergies and autoimmune diseases’ incidence.3 Birth mode has been shown to impact microbiota.2 Korpela et al showed that a higher level of the HMO 2’fucosylactose (2’FL) may alleviate the efects of caesarian birth on gut microbiota.4 In a randomized double-blinded controlled trial, 63 healthy infants received infant formula (control) and were compared to 58 infants fed the same formula with added two HMOs.
At 3 months of age, microbiota composition in the test group appeared closer to that of breastfed neonates.5 In a study of 500 samples of milk from 25 mothers breastfeeding very preterm infants and 28 mothers breastfeeding term infants, Austin et al showed that the concentrations of a number of HMOs were signifcantly lower in preterm compared to term milk.6 Preterm infants’ morbidity such as necrotizing enterocolitis and late onset sepsis have been shown to be associated with HMO milk content.3,7 The question arises of a beneft of HMO supplementation on microbiota in premature infants?
To address that question, a multicenter randomized controlled intervention study of the efect of a supplement containing 2 HMOs (2’FL and LNnT at 0.34 and 0.034 g/Kg/day respectively) in very preterm infants was set up. The primary objective was to demonstrate feeding tolerance measured by non-inferiority in days to reach full enteral feeding (FEF). Secondary outcome included growth parameters, gastro-intestinal symptoms, adverse events up to 12 months corrected age, fecal microbiota, gut maturation/immune biomarkers and breastmilk HMO content. Administration of the products occured after 24 hours trophic feeding and within the frst 5 days postnatal age (Figure).
Figure : Intervention study protocol
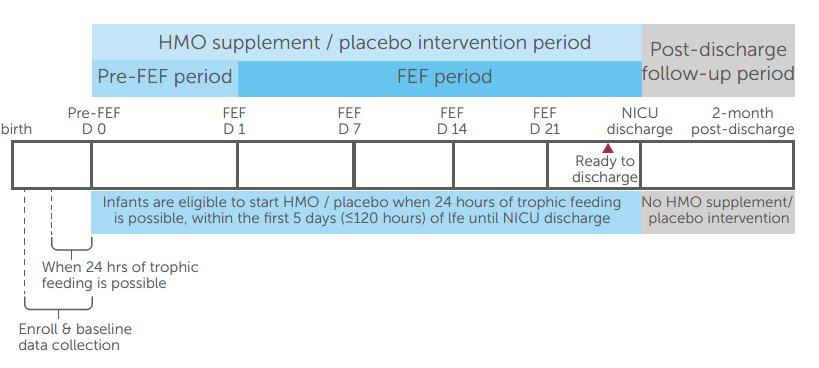
FEF was defined as both enteral feeding volume of at least 150ml/Kg/day and parenteral nutrition discontinuation.
Forty-three infants were included in each group. Gestational age was (Mean ± Standard deviation) 29.7±1.4 vs. 30.2±1.4 weeks. Both groups were comparable for weight, length and head circumference for age z-scores. There was no difference for the sex ratio or caesarian section delivery. The primary objective was achieved and no significant difference was observed for any adverse event.
In conclusion, in premature infants, gut microbiota may show different patterns related with NICU practices and maturity, and may be associated with the outcome. Microbiota appears to be associated with lower level of HMOs in breastmilk in preemies. Specific HMOs milk content may be associated with short and long term clinical outcome. HMO supplementation that might show a benefit for dysbiosis reduction leading to more mature microbiota is under investigation
Thank you to Yipu Chen, Nestlé Product Technology Center - Nutrition, Vevey, Switzerland, for her contribution to this abstract.
References
1. Harmsen HJM, Wildeboer–Veloo ACM, Raangs GC, et al. Analysis of Intestinal Flora Development in Breast- Fed and Formula-Fed Infants by Using Molecular Identifcation and Detection Methods: J Pediatr Gastroenterol Nutr. janv 2000;30(1):61-7.
2. Rozé J-C, Ancel P-Y, Marchand-Martin L, et al. Assessment of Neonatal Intensive Care Unit Practices and Preterm Newborn Gut Microbiota and 2-Year Neurodevelopmental Outcomes. JAMA Netw Open. 23 sept 2020;3(9):e2018119.
3. Masi AC, Embleton ND, Lamb CA, et al Human milk oligosaccharide DSLNT and gut microbiome in preterm infants predicts necrotising enterocolitis. Gut. 2020 doi: 10.1136/gutjnl-2020-322771.
4. Korpela K, Salonen A, Hickman B, et al. Fucosylated oligosaccharides in mother’s milk alleviate the effects of caesarean birth on infant gut microbiota. Sci Rep. déc 2018;8(1):13757.
5. Berger B, Porta N, Foata F, et al. Linking Human Milk Oligosaccharides, Infant Fecal Community Types, and Later Risk To Require Antibiotics. Pettigrew MM, éditeur. mBio. 17 mars 2020;11(2):e03196-19, / mbio/11/2/mBio.03196-19.atom.
6. Austin S, De Castro CA, Sprenger N et al. Human Milk Oligosaccharides in the Milk of Mothers Delivering Term versus Preterm Infants. Nutrients. 5 juin 2019;11(6):1282.
7. Morrow AL, Meinzen-Derr J, Huang P, et al . Fucosyltransferase 2 non-secretor and low secretor status predicts severe outcomes in premature infants. J Pediatr. 2011 May;158(5):745-51. doi: 10.1016/j. jpeds.2010.10.043. Epub 2011 Jan 22. PMID: 21256510; PMCID: PMC3412418
If you liked this post you may also like