Globally, early preterm birth is a leading cause of death in children under 5 years of age. Initial observations on the longer duration of pregnancies and reduced incidence of preterm birth in fish-eating communities prompted further research into the role of omega-3 (n-3) long-chain polyunsaturated fatty acids (LCPUFA) in improving gestation length. The prenatal period is a vulnerable window that is highly sensitive to n-3 LCPUFA deficiency.
Current knowledge
The majority of preterm births occur spontaneously and are due to multiple factors that trigger the normally quiescent uterus to undergoing contractions and labor. Currently, there is no strategy that can be used as a primary prevention for widespread clinical use. The n-3 LCPUFA such as docosahexaenoic acid (DHA) and eicosapentaenoic acid are dietary agents that can modulate several clinical conditions via their anti-inflammatory actions. These may be relevant for modulating the inflammatory cascades that underpin the maternal response to the fetus during the birth process.
Practical implications
The most compelling evidence to support the efficacy of DHA supplementation in reducing preterm birth came from the DOMInO trial. Supplementation of n-3 LCPUFA during the last half of pregnancy in 2,399 women resulted in a 50% reduction in the incidence of early preterm birth. These findings have been supported by those from several other trials and meta-analyses. In general, supplementation with marine oil or n-3 LCPUFA in pregnancy is safe and well tolerated, but further work needs to be done to clarify the optimal dosage and timing of n-3 supplementation during pregnancy.
Recommended reading
Makrides M, Gibson RA, McPhee AJ, et al: Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: a randomized controlled trial. JAMA 2010;304:1675–1683.
Preterm birth is one of the leading causes of infant deaths worldwide. There is a growing need to identify safe, effective, easily available primary prevention strategies to prevent preterm delivery, especially ‘early preterm birth’ before 34 weeks of gestation.
Epidemiological and randomised controlled trial evidence exists to support an effect of increased omega-3 long-chain polyunsaturated fatty acid intake during pregnancy on length of gestation.
Preterm birth accounts for more than 85% of all perinatal complications and deaths. There are many short- and longterm consequences of being born too soon. These infants often require intensive care and are at increased risk of early morbidities often with life-long sequelae. Approximately 50% of all preterm births have unknown or unclear causes, and there are no effective primary prevention strategies in widespread clinical use. Epidemiological studies have observed an increased length of gestation in populations with high fish consumption. These findings have led to randomised controlled trials of omega-3 (n-3) long-chain polyunsaturated fatty acid (LCPUFA) supplementation which show that these dietary agents may delay the timing of birth and may have value as a prophylactic intervention in some women. This review presents the available evidence and discusses the relationship between prenatal n-3 LCPUFA supplementation during pregnancy and the incidence of preterm birth.
Introduction
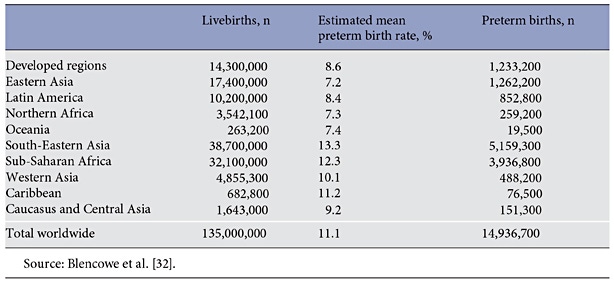
Preterm birth (before 37 completed weeks of gestation) complications are now the leading cause of underfive deaths globally, accounting for 17% of all such deaths [1] and more than 85% of all perinatal complications [2]. It is estimated that 11% of births (15 million babies each year worldwide) are premature (table 1), with half of these due to unknown or unclear causes [3–5]. Advances in perinatal and neonatal care have resulted in greatly improved survival rates for preterm babies; however, there is an increasing awareness that, even in high-income countries, many of these children suffer short- and longterm consequences of being born too soon [6]. These infants often require intensive care and are at increased risk of early morbidities such as respiratory distress syndrome, intraventricular haemorrhage, necrotising enterocolitis, blindness and cerebral palsy. In early childhood, developmental difficulties may emerge in preterm children and later manifest as low educational achievement, high unemployment and other deficits in social and emotional wellbeing, as well as having wider societal and economic impacts [7, 8].
Table 1. Estimated preterm birth rates and total number of preterm births for 2010
One quarter of preterm births are due to medical intervention following pregnancy-related complications including pre-eclampsia, intra-uterine growth restriction or maternal disease [9] . The remainder of preterm births occur spontaneously and are due to multifactorial processes causing the uterus to change from quiescence to active contractions and birth. The precise cause of spontaneous preterm labour is of unknown aetiology in up to half of all cases [10] . Whilst tocolytic drugs to inhibit uterine contractions are available in an emergency situation to stop or delay premature labour, there are currently no effective primary prevention strategies for preterm birth in widespread clinical use. More than 10 Cochrane systematic reviews have investigated treatments ranging from dietary supplements to therapeutic drugs such as betamimetics, magnesium sulphate and calcium channel blockers. Despite the wide range of treatments investigated in the reviews, none have been shown to be effective in reducing the risk of spontaneous preterm birth.
n-3 LCPUFA and Preterm Birth
In recent decades, omega-3 (n-3) long-chain polyunsaturated fatty acids (LCPUFA), specifically docosahexaenoic acid (DHA, 22: 6n-3) and eicosapentaenoic acid (EPA, 20: 5n-3), have emerged as efficacious dietary agents that moderate a number of clinical conditions through their known anti-inflammatory activity. This action may also apply to pregnancy and the inflammatory cascade of labour where the maternal immune response to the fetus is crucial. The feto-placental unit is supplied with n-3 and omega-6 (n-6) LCPUFA from the maternal circulation, which is influenced by maternal dietary intake and endogenous synthesis. The prostaglandins derived from n-6 arachidonic acid (AA, 20: 4n-6) within the utero-placental unit in normal pregnancy are countered by local production of prostaglandins derived from n-3 LCPUFA within the same tissues. The balance between the metabolites of n-3 and n-6 fatty acids plays an important role in the maintenance of normal gestation length and is a critical element in cervical ripening and the initiation of labour [11]. If local production of n-6-derived prostaglandins within the feto-placental unit is too high, or local accumulation of n-3 LCPUFA is too low, the cervix may prematurely ripen and uterine contractions increase, which may in turn lead to preterm birth, particularly in susceptible women [12].
Maternal DHA Intake
Modern Western diets are low in n-3 LCPUFA and high in n-6 fatty acids, leading to a predominance of AA in tissues. The prenatal period is a time of increased risk for n-3 LCPUFA deficiency as DHA is preferentially transferred from maternal tissue stores to the developing fetus [13]. The World Health Organization recommends an intake of 300 mg/day of n-3 LCPUFA for pregnant women [14]; however, women in many low-, middle- and high-income countries do not achieve this amount, with the exception of coastal countries where fish and other marine foods are easily accessible, affordable and commonly consumed [15]. Whilst marine foods are rich sources of DHA and EPA, nutritional advice for pregnant women regarding marine oil consumption is complicated with warnings that suggest limiting overall fish consumption to avoid potential methyl-mercury or polychlorinated biphenyls exposure. As a result, the intake of these long-chain n-3 fats is well below the required intake to achieve normal rises in the feto-placental unit for the maintenance of a full-term pregnancy, highlighting a potential insufficiency for the feto-placental unit. This has been suggested to contribute to the increasing rate of preterm birth in developed countries, as well as in the developing countries where diets have become more Westernised with lower intakes of fish and higher intake of n-6-rich vegetable oils [16].
Epidemiological Evidence
The first observations linking n-3 LCPUFA intake and pregnancy duration were made following population comparisons in the early 1980s. The longer duration of pregnancies observed in the genetically similar fish-eating community of the Faroe Islands compared to Danish women led to the suggestion that fatty acids from marine food, a rich source of EPA and DHA, could delay spontaneous delivery [17]. Subsequent cohort studies have also demonstrated a positive association between fish or n-3 LCPUFA intake and the duration of gestation [18–20]. A systematic review of 151,880 mother-child pairs from 19 population-based European birth cohort studies showed that women who ate fish >1 time/week during pregnancy had a lower risk of preterm birth than women who rarely ate fish [21]. The apparent consistency of these associations appears promising; however, it is not possible to infer a causal link between increased n-3 LCPUFA exposure (via fish) in pregnancy and increased gestational length because of the difficulty in excluding the possibility of residual confounding environmental factors, or that there may be constituents of fish other than n-3 LCPUFA driving these associations.
It is not possible to infer a causal link between increased n-3 LCPUFA exposure (via fish) in pregnancy and increased gestational length because of the difficulty in excluding the possibility of residual confounding environmental factors
Evidence from Randomised Controlled Trials
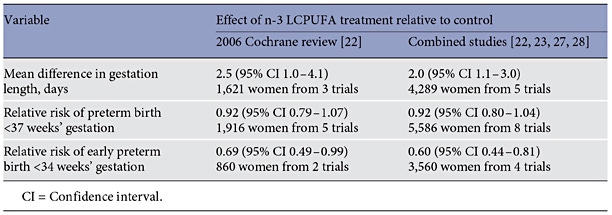
Initial randomised controlled trials (RCTs) investigating the effect of n-3 LCPUFA supplementation for the prevention of preterm birth used high-dose EPA-rich fish oil and largely targeted women with higher-risk pregnancies. A 2006 Cochrane review of marine oil supplementation during pregnancy included data from 6 trials and measured a variety of maternal and neonatal health outcomes including preterm birth [22]. Two of these trials (n = 860 women in total) measured preterm birth outcomes of women with high-risk pregnancies. A meta-analysis showed that the fish oil intervention resulted in an approximate 2-day increase in the mean duration of gestation, a nonsignificant 8% reduction in preterm birth <37 weeks’ gestation and a significant 31% reduction in early preterm birth <34 weeks’ gestation. More recent trials of prenatal n-3 supplementation have included women with normal-risk pregnancy and have intervened with DHA because of the association with early childhood developmental outcomes [23–25]. The strongest evidence to support the efficacy of DHA supplementation to reduce preterm birth comes from the DOMInO trial, the largest trial to date of n-3 LCPUFA supplementation in pregnancy (n = 2,399) [23]. This trial was designed to assess the effect of n-3 LCPUFA supplementation (predominantly as DHA) during the last half of pregnancy on the prevalence of postnatal depression in women and on early childhood neuro-developmental outcomes. A preplanned secondary analysis showed a reduction in early preterm birth (<34 weeks) in the DHA-supplemented group compared with the control group, corresponding to a 50% reduction in the incidence of early preterm birth (1.09 vs. 2.25%, adjusted RR 0.49, 95% CI 0.25–0.94, p = 0.03). These findings concur with results of the 2006 Cochrane review, and when combined in an updated meta-analysis including two other trial recent trials (n = 3670) [24, 26], the numbers of included women increase 2.5- to 3-fold and the effect sizes remain remarkably similar and are increasingly compelling (table 2).
Table 2. Cochrane review of n-3 LCPUFA for the prevention of preterm birth
Collectively, data from the Cochrane systematic review [22] combined with more recent reviews [27–29] imply that the effects of n-3 LCPUFA are not attributable only to prostaglandins arising from EPA, as newer trials have used DHA-based supplementation. Clearly the mechanisms underlying the effects of n-3 LCPUFA on the duration of gestation are complex, and this is perhaps not surprising when one considers that multiple mechanisms often underpin important biological processes, and it is likely that birth is no exception. Doses of n-3 LCPUFA supplementation used in RCTs during pregnancy range from 133 to 3,000 mg/day, and the intervention period has commenced between 16 and 30 weeks’ gestation until delivery or beyond. Overall, systematic reviews show that supplementation with marine oil or n-3 LCPUFA is safe in pregnancy and is generally well tolerated. Rates of serious adverse events were similar between treatment groups and occurrence of side effects (e.g. vomiting, nausea and diarrhoea) was generally similar except for belching and bad taste, which occurred more frequently in the marine oil-supplemented groups. No differences have been shown in the incidence of antepartum hospitalisation, caesarean section, eclampsia or other serious maternal morbidity between treatment and control groups [22, 27, 28]. However, a number of trials did report a significant increase in the incidence of post-term inductions or post-term pre-labour caesarean section in women supplemented with n-3 LCPUFA until delivery compared with control. This is a concern because post-term birth is also associated with increased perinatal mortality and morbidity in both infants and mothers [30]. Animal studies demonstrate that as the duration, dose and timing of n-3 LCPUFA supplement administration are altered, the levels accumulated within the feto-placental unit change in a timed dose-response relationship [11]. It has been shown that within 6 weeks, people who stop taking fish oil supplements have their plasma and red cell n-3 LCPUFA return to levels which are similar to those of the general population of low fish consumers [31]. Current trials are investigating the optimal timing of n-3 LCPUFA supplementation targeting the critical period before 34 weeks when preterm delivery has the poorest outcomes and ceasing treatment to reduce the risk of post-term intervention (Australian New Zealand Clinical Trials Registry number 12613001142729).
Conclusions
Preventing preterm birth remains one of the most challenging issues in obstetric and neonatal care. Whilst a level of concordance is evident between epidemiological studies and RCTs, inconsistencies remain. This is perhaps not surprising when one considers that maternal n-3 LCPUFA exposure in observational studies is most likely based on a lifetime of exposure compared to a defined period of n-3 LCPUFA supplementation in RCTs. The evidence to date consistently demonstrates that n-3 LCPUFA supplementation during pregnancy increases the mean duration of gestation by 2 days and produces a 40–50% reduction in early preterm birth (<34 weeks’ gestation) [22, 23]. Future directions for research in this area include refinement of dosing and timing of n-3 LCPUFA supplementation. It is important to identify and evaluate (by RCT) other agents and sustainable food-based dietary interventions that are thought to influence similar pathways. In addition, further studies to understand the mechanisms surrounding individual response to n-3 LCPUFA supplementation and the relationship to immune profile/inflammatory indicators, as well as social and clinical characteristics will be vital in optimising future treatment recommendations.
Disclosure Statement
The writing of this article was supported by Nestlé Nutrition Institute. Maria Makrides was supported by an Australian National Health and Medical Research Council Senior Research Fellowship (1061704). Karen Best declares that she has no relevant or material financial interests that relate to the research described in this paper.
References
World Health Statistics 2015. Geneva, World Health Organization, 2015. http://www.who. int/gho/publications/world_health_statistics/ 2015/en/ (accessed April 20, 2016).
Kong W, Yen JH, Ganea D: Docosahexaenoic acid prevents dendritic cell maturation, inhibits antigen-specific Th1/Th17 differentiation and suppresses experimental autoimmune encephalomyelitis. Brain Behav Immun 2011; 25: 872–882.
Schober L, Radnai D, Schmitt E, Mahnke K, Sohn C, Steinborn A: Term and preterm labor: decreased suppressive activity and changes in composition of the regulatory Tcell pool. Immunol Cell Biol 2012; 90: 935– 944.
Novak TE, Babcock TA, Jho DH, Helton WS, Espat NJ: NF-kappa B inhibition by omega-3 fatty acids modulates LPS-stimulated macrophage TNF-alpha transcription. Am J Physiol Lung Cell Mol Physiol 2003; 284: L84–L89.
Martinez FO, Helming L, Gordon S: Alternative activation of macrophages: an immunologic functional perspective. Annu Rev Immunol 2009; 27: 451–483.
Saigal S, Doyle LW: An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008; 371: 261–269.
Catov JM, Bodnar LM, Olsen J, Olsen S, Nohr EA: Periconceptional multivitamin use and risk of preterm or small-for-gestational- age births in the Danish National Birth Cohort. Am J Clin Nutr 2011; 94: 906– 912.
McPartlin J, Halligan A, Scott JM, Darling M, Weir DG: Accelerated folate breakdown in pregnancy. Lancet 1993; 341: 148–149.
Bennett P, Thornton S: Preterm labour. Preface. Best Pract Res Clin Obstet Gynaecol 2007; 21: 727–728.
Menon R, Bonney E: Oxidative stress and preterm birth; in Dennery PA, Buonocore G, Saugstad OD (eds): Perinatal and Prenatal Disorders. New York, Springer, 2014, pp 95– 115.
Brazle A, Johnson B, Webel S, Rathbun T, Davis D: Omega-3 fatty acids in the gravid pig uterus as affected by maternal supplementation with omega-3 fatty acids. J Anim Sci 2009; 87: 994–1002.
Simopoulos AP: The importance of the omega- 6/omega-3 fatty acid ratio in cardiovascular disease and other chronic diseases. Exp Biol Med (Maywood) 2008; 233: 674–688.
Makrides M, Gibson RA: Long-chain polyunsaturated fatty acid requirements during pregnancy and lactation. Am J Clin Nutr 2000; 71(1 suppl):307S–311S.
Astrup AV: Fats and fatty acids in human nutrition. Report of an expert consultation. Geneva, Food and Agriculture Organization of the United Nations (FaAOotU), 2010.
Koletzko B, Lien E, Agostoni C, Bohles H, Campoy C, Cetin I, et al: The roles of longchain polyunsaturated fatty acids in pregnancy, lactation and infancy: review of current knowledge and consensus recommendations. J Perinat Med 2008; 36: 5–14.
McGregor JA, Allen KG, Harris MA, Reece M, Wheeler M, French JI, et al: The omega- 3 story: nutritional prevention of preterm birth and other adverse pregnancy outcomes. Obstet Gynecol Surv 2001; 56(5 suppl 1):S1–S13.
Olsen SF, Hansen HS, Secher NJ, Jensen B, Sandstrom B: Gestation length and birth weight in relation to intake of marine n-3 fatty acids. Br J Nutr 1995; 73: 397–404.
Muthayya S, Dwarkanath P, Thomas T, Ramprakash S, Mehra R, Mhaskar A, et al: The effect of fish and omega-3 LCPUFA intake on low birth weight in Indian pregnant women. Eur J Clin Nutr 2009; 63: 340–346.
Olsen SF: Low consumption of seafood in early pregnancy as a risk factor for preterm delivery: prospective cohort study. BMJ 2002; 324: 447.
Oken E, Kleinman KP, Olsen SF, Rich-Edwards JW, Gillman MW: Associations of seafood and elongated n-3 fatty acid intake with fetal growth and length of gestation: results from a US pregnancy cohort. Am J Epidemiol 2004; 160: 774–783.
Leventakou V, Roumeliotaki T, Martinez D, Barros H, Brantsaeter AL, Casas M, et al: Fish intake during pregnancy, fetal growth, and gestational length in 19 European birth cohort studies. Am J Clin Nutr 2014; 99: 506– 516.
Makrides M, Duley L, Olsen Sjurdur F: Marine oil, and other prostaglandin precursor, supplementation for pregnancy uncomplicated by pre-eclampsia or intrauterine growth restriction. Cochrane Database Syst Rev 2006; 3:CD003402.
Makrides M, Gibson RA, McPhee AJ, Yelland L, Quinlivan J, Ryan P, et al: Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: a randomized controlled trial. JAMA 2010; 304: 1675–1683.
Carlson SE, Colombo J, Gajewski BJ, Gustafson KM, Mundy D, Yeast J, et al: DHA supplementation and pregnancy outcomes. Am J Clin Nutr 2013; 97: 808–815.
Ramakrishnan U, Stein AD, Parra-Cabrera S, Wang M, Imhoff-Kunsch B, Juarez-Marquez S, et al: Effects of docosahexaenoic acid supplementation during pregnancy on gestational age and size at birth: randomized, double-blind, placebo-controlled trial in Mexico. Food Nutr Bull 2010; 31(2 suppl): S108–S116.
Ramakrishnan U, Grant F, Goldenberg T, Zongrone A, Martorell R: Effect of women’s nutrition before and during early pregnancy on maternal and infant outcomes: a systematic review. Paediatr Perinat Epidemiol 2012; 26: 285–301.
Szajewska H, Horvath A, Koletzko B: Effect of n–3 long-chain polyunsaturated fatty acid supplementation of women with low-risk pregnancies on pregnancy outcomes and growth measures at birth: a meta-analysis of randomized controlled trials. Am J Clin Nutr 2006; 83: 1337–1344.
Horvath A, Koletzko B, Szajewska H: Effect of supplementation of women in high-risk pregnancies with long-chain polyunsaturated fatty acids on pregnancy outcomes and growth measures at birth: a meta-analysis of randomized controlled trials. Br J Nutr 2007; 98: 253–259.
Kar S, Wong M, Rogozinska E, Thangaratinam S: Effects of omega-3 fatty acids in prevention of early preterm delivery: a systematic review and meta-analysis of randomized studies. Eur J Obstet Gynecol Reprod Biol 2016; 198: 40–46.
NICE clinical guidelines 70: Induction of labour. National Institute for Health and Clinical Excellence. 2008. https://www.rcog. org.uk/en/guidelines-research-services/ guidelines/induction-of-labour-nice-clinical- guideline-70/ (accessed April 24, 2016).
Lumley J: Defining the problem: the epidemiology of preterm birth. BJOG 2003; 110(suppl 20):3–7.
Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller A-B, Narwal R, et al: National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 2012; 379: 2162–2172.