The scientific basis for healthful carbohydrate profile
Different solutions can be used to replace sugars in food products but it is important to ensure that these solutions are more healthful than the sugars they replace. The objectives of this paper are, (1) to identify carbohydrates and carbohydrates sources to promote and those to limit for dietary intake and food product development, based on current knowledge about the impact of carbohydrates on the development of dental caries, obesity and cardiometabolic disorders (2) to evaluate the impact of food processing on the quality of carbohydrates and (3) to highlight the challenges of developing healthier products due to the limitations and gaps in food regulations, science & technology and consumer education.
Introduction
Dietary carbohydrate should provide 45–65% of total energy intake (Institute of Medicine 2005, EFSA journal 2010). Accordingly, carbohydrates (see classification, Table 1) represent the main macronutrient in most people’s diets. Among the different carbohydrates, sugars have been the subject of a lot of attention. In 2010, the European Food Safety Authority (EFSA) recognized the role of added sugars in the risk of developing dental caries, obesity and type 2 diabetes (T2D), but indicated that the available data were insufficient to set an upper limit of intake (Table 2). In 2015, the World Health Organization (WHO) set upper limits by recommending that the intake of
free sugars be less than 10% of the total energy intake (strong recommendation) and a further reduction to less than 5% of total energy intake (conditional recommendation) throughout the lifespan for preventing both dental caries and obesity(Table 2). The US Dietary Guidelines Advisory Committee (DGAC) has also proposed a 10% upper limit for added sugars intake (Table 2). More recently, the Scientific Advisory Committee on Nutrition (SACN) has associated sugars and foods containing sugars with a greater risk of tooth decay and increase in body weight, resulting in a recommendation of free
sugars intake of less than 5% of total energy (Table 2).
In order to achieve this public health target, consumers will need to make significant changes to their diets. At the same time, it results in the need to develop healthful technological solutions to reduce sugars in packaged foods. Different solutions can be applied to replace sugars to help consumers to follow dietary guidelines, but it is important to ensure that they are truly supportive of the expected health benefits, i.e, contribution to reduce the risk of dental caries, obesity, T2D and vcardiovascular diseases (CVD). For that reason, it is pertinent to develop healthful carbohydrate blends, possibly by using better sources of carbohydrates and avoiding ultra-processing of
manufactured products. However, in order to achieve this shift, some major limitations and scientific gaps need to be overcome.
Dietary carbohydrates, health & diseases
Recently, the current evidence of the role of dietary simple and complex carbohydrates in the development of four public health issues, i.e, dental caries, obesity, T2D and CVD have been extensively reviewed through systematic review or metaanalysis (SACN 2015). However, some of the evidence that describes the negative impact of excessive intake of sugars on health is based on association studies, not proving causality. It is therefore important to identify the potential mechanisms of action for the postulated health effects to reinforce further support the plausibility of the observed associations and the various intrinsic properties of the carbohydrates linked to a specific health outcomes.
Dental caries
Dental caries occur due to tooth demineralization by organic acids produced by the combination of orally fermentable carbohydrates (e.g., glucose, sucrose, digestible oligosaccharides and starches) and dental plaque bacteria (Moynihan and Petersen
2004). Therefore, the main property linking a given sugar or complex carbohydrate to dental caries is their fermentability by specific bacteria in the oral cavity.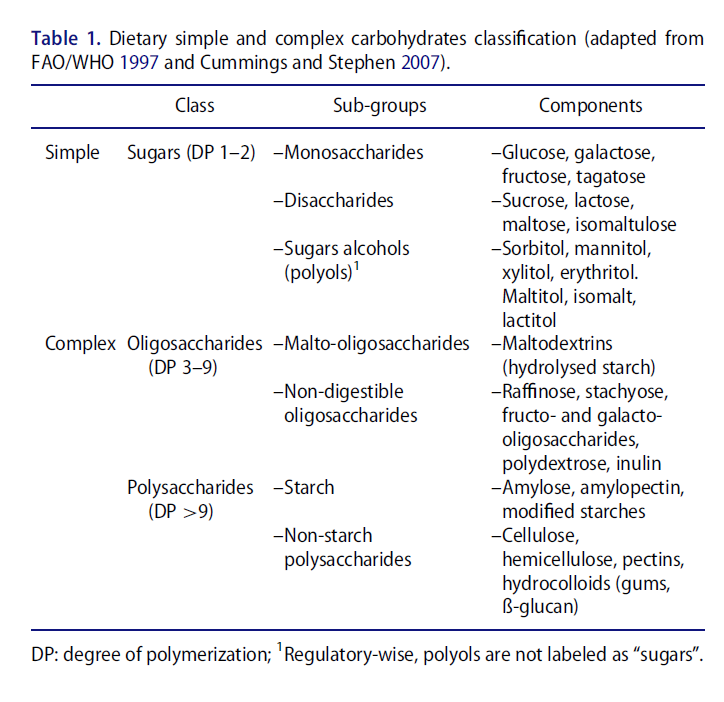
Sugars (mono- and disaccharides)
Both cohort studies and human trials have shown an association between the consumption of total sugars and foods or beverages containing sugars with a greater risk of dental caries (SACN 2015). Among the sugars, there is no clear evidence of
differences in the cariogenicity between fructose, glucose and sucrose. However, lactose is fermented more slowly in the oral cavity than sucrose (Birkhed et al. 1993). In agreement, early studies of plaque pH in human subjects have shown that plaque bacteria produce less acid from lactose compared with other sugars (Jenkins and Ferguson 1966). Interestingly, rare sugars, such as tagatose (an isomer of fructose) and isomaltulose (a structural isomer of sucrose) are recognized to be non cariogenic and have obtained an EFSA positive opinion and health claim approval by the US Food & Drug Administration (FDA) on the prevention of dental caries when replacing sucrose (EFSA 2011; FDA 2017). However, under food regulations, tagatose and isomaltulose are not exempted from the definition of sugars. This means that they are labeled as such and counted as free/added sugars when used in food manufacturing. Interestingly, sugar alcohols (e.g., xylitol and sorbitol), which have been also shown to be non-cariogenic (Hayes 2001) and are associated to positive dental health claims in Europe (EFSA 2011) and in the US (FDA 2017) are not declared as added sugars but under total carbohydrates.
Oligo- and polysaccharides
The cariogenenicity of digestible oligo- and polysaccharides has been less extensively studied. Nevertheless, there is some evidence that foods rich in maltodextrins (starch partially hydrolyzed) (Levine 1998; Al-Khatib et al. 2001) or rapidly digested starches (e.g., highly gelatinized) (Lingstr€om et al. 2000) may also contribute to dental caries, since easily available to salivary enzymes, which results in maltose and to a lesser extent, glucose release. Therefore, depending on the residence time in the mouth and the nature and extent of chewing, some complex carbohydrates, such as maltodextrins, might have a non negligeable cariogenicity. To our knowledge, non-digestible oligo-
(e.g., fructo- and galacto-oligosaccharides) and polysaccharides have not been reported to be cariogenic.
Key messages:
–Not all sugars are cariogenic (e.g., tagatose, isomaltulose)
–Some complex carbohydrates, but not fibers, might be cariogenic
Obesity
Obesity is an excess of body fat that occurs when energy intake from foods is greater than total energy expenditure during a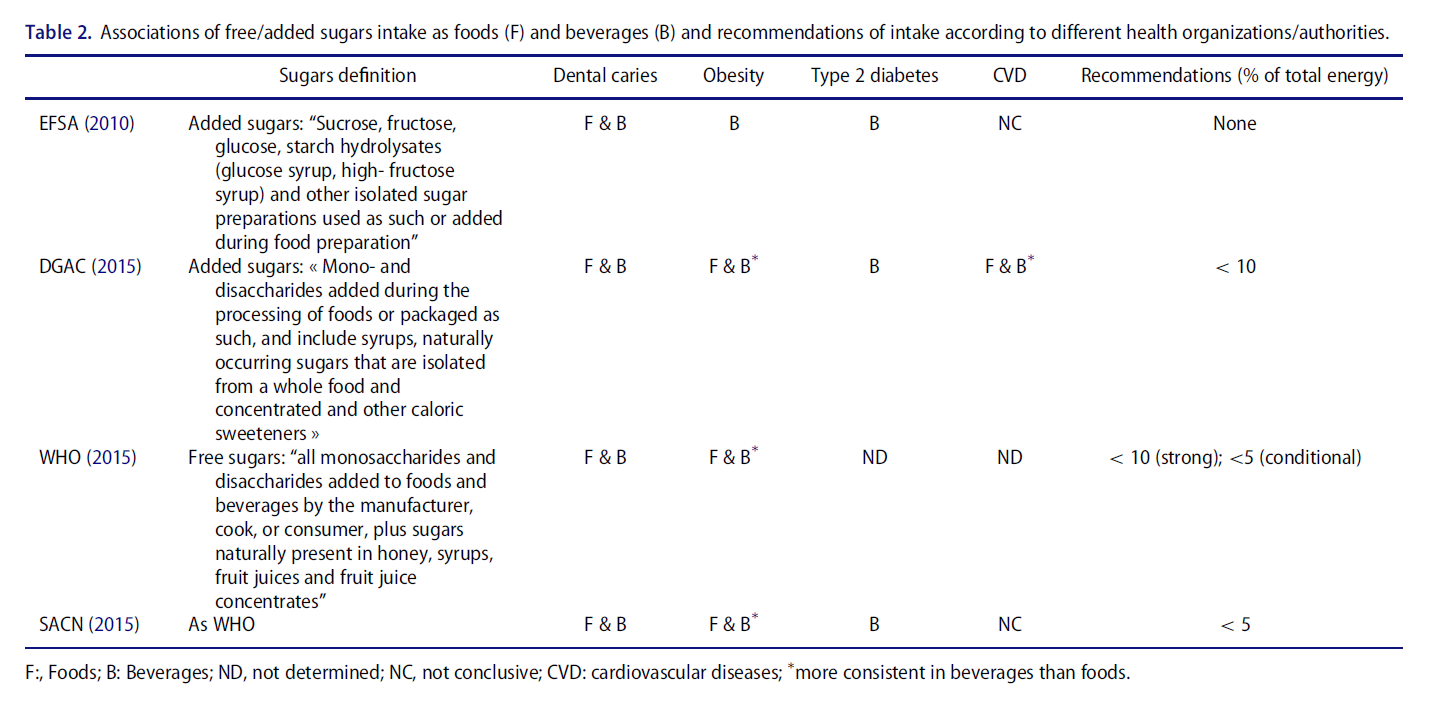
prolonged period of time. Therefore, the main property linking a given sugar or complex carbohydrate to obesity is their caloric content.
Sugars
A meta-analysis of randomized controlled trials indicates that reducing or increasing intake of free sugars promotes, respectively, loss or gain in body weight (Te Morenga et al. 2012). However, no evidence of difference in body weight change was found when the group interventions were isocaloric through isoenergetic exchanges of dietary sugars with other carbohydrates or other macronutrient sources. This suggests that calories, rather than the sugars per se, are the main driver of the body weight gain. Indeed, there is a growing consensus that high intake of free/added sugars, especially in sugars-sweetened beverages, increases overall energy intake. The mechanism behind this calorie overconsumption might be different between liquids and solid foods. Today, most of the evidence linking sugars and obesity have involved sugars-sweetened beverages
rather than solid foods. The mechanism might be explained by the less satiating effect of liquid vs solid foods (DiMeglio and Mattes 2000; de Graaf 2011). Regarding solid foods, the potential mechanism is less clear. It has been proposed that foods rich in sugars are also often high in energy density (Te Morenga et al. 2014) and that such foods are less
satiating than those that are less energy dense (Rolls 2009). One potential direct role of sugars might come from its sweetness, even though the role of sweet taste in energy intake and appetite regulation in humans is controversial (Yeomans 2012). This research field certainly deserves more attention, and will be key to drive nutritional recommendations and product (re) formulation strategies.
Sugar alcohols being less absorbed than sugars show a lower energy density, ranging from 0.2 to 3 kcal/g (Livesey 2003). Consequently, they can reduce the energy density of a food and potentially calorie intake, when used as sugar replacer.
Oligo- and polysaccharides
Regarding the risk of obesity, there is no evidence, when total energy is matched and in excess, that digestible oligo- and polysaccharides are less detrimental than sugars. Maltodextrins, which are commonly used in beverages (Hofman et al. 2016), have the same caloric value as glucose or sucrose but a lower sweetness (Table 3).
Dietary fibers provide few calories and almost no sweetness (Table 3). Consequently, they represent a good alternative for reducing the energy density of certain foods and the risk of overconsumption. Indeed, some randomized control trials have shown a positive association between dietary fiber intake, as foods or supplements, and weight loss. Several cohort studies have also shown an inverse association with weight gain (EFSA 2010). However, using a more systematic search strategy, the SACN (SACN 2015) has recently concluded that at present there is no consistent evidence of an association between dietary fiber intake and body weight change.
Key messages:
–High intake of free/added sugars is associated with higher risk of obesity, particularly when consumed under liquid form
–The potential underlying mechanisms seem to favor an indirect role of sugars and highlight the issue of caloric beverages and energy dense foods
–Some sugars (e.g., allulose and tagatose) have lower caloric value than 4 kcal/g
–The role of sweetness as a potential contributor of calorie overconsumption deserves further investigation
–Intake of dietary fibers might have some protective effects against weight gain
Type 2 diabetes
T2D is characterized by the body’s inability to respond to insulin action and/or produce enough insulin, which causes elevated levels of glucose in the blood (hyperglycemia). Obesity is a major risk factor for the development of T2D and CVD (Pi-Sunyer 1991). The sequence of biological events that leads from obesity to T2D and CVD is known (Saltiel and Olefsky 1996). Briefly, excess adipose tissue, especially visceral fat, promotes insulin resistance, which may lead to impaired glucose tolerance characterized by an excessive glycemic response (GR) after carbohydrate ingestion. The transition from this prediabetic state to T2D can take many years and is often associated with a decline in the capacity of beta cells to secrete enough insulin (Fonseca 2009). The potential role of carbohydrates in the development of T2D is their ability to increase glycemic and inulinemic response after ingestion. The postprandial GR can be translated into a standardized index (Jenkins et al. 1981), which allows the ranking of different carbohydrates or carbohydrate-containing foods on a scale called the glycemic
index (GI). The lower and higher the GI is, a lower and higher GR is expected, respectively. In addition, the glycemic load (GL), calculated as the product of GI and the quantity of available carbohydrates in a serving of the test food (divided by 100) estimates both the “quality” and the quantity and therefore represents a better proxy of GR than GI (Salmeron et al. 1997). Mirroring the GI concept, the insulin index (II) was developed to quantify the postprandial insulin response to different carbohydrates or foods (Holt et al. 1997). The II values for carbohydrate and food correlate with their GI (low GI → low II high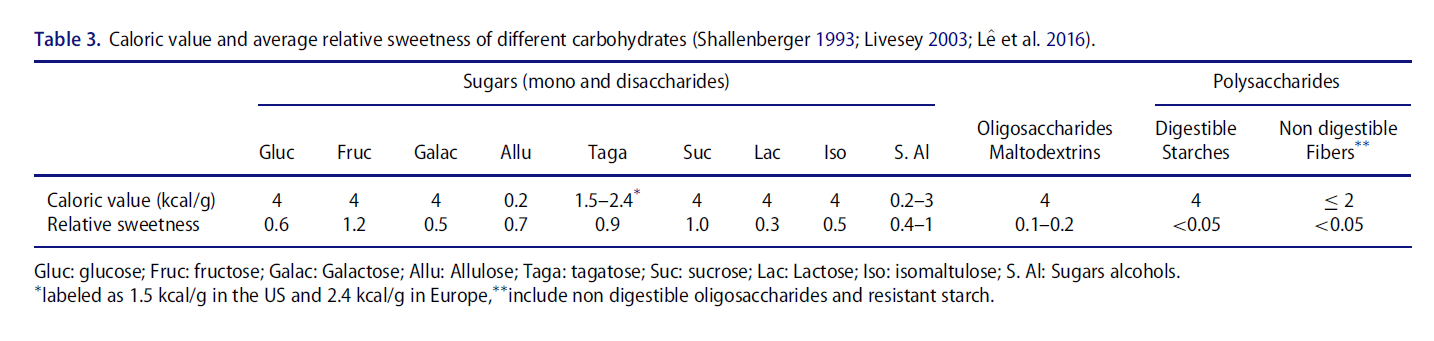
GI → high II), with some exceptions for foods containing high levels of proteins, especially dairy proteins, where a low GI can be associated to a higher II than expected.
Sugars
The association between free/added sugars and T2D was not addressed by the WHO but it was addressed by the US dietary and the UK nutrition advisory committees (DGAC and SACN, respectively). These committees found moderate to strong evidence associating an increased risk of T2D with a higher consumption of free/added sugars in the form of sugars-sweetened beverages (SACN 2015, DGAC 2015). According to the DGAC, this relationship is not completely explained by change in body weight. One potential mechanism by which the excess of sugars consumption might promote the development of T2D, independently of overweight and obesity, is the capacity of certain
sugars to trigger a high postprandial glycemic or insulinemic response. However, not all sugars will promote a high GR as indicated by their GI (Table 4); glucose and sucrose triggering the highest response, lactose, isomaltulose, fructose and galactose an intermediate one, while tagatose and allulose having almost no effect on blood glucose levels.
Sugar alcohols have lower GI and II than glucose or sucrose (Livesey 2003) and therefore represent a good alternative to limit the glycemic and insulinemic response of a food. In 2011, their use as sugar replacers received a positive opinion from EFSA for their property to decrease the glycemic response (EFSA 2011).
Oligo- and polysaccharides
Based on cohort studies, no association was found between total starch intake and T2D. But this analysis does not take into account the different types of starch i.e., rapidly or slowly digested starches. Interestingly, when starchy foods are considered, some cohort studies have associated high consumption of cooked potatoes and rice (white but not brown) with higher incidence of T2D (Halton et al. 2006 Hu et al. 2012). As shown in Table 4, complex carbohydrates such as malto-oligosaccharides and some starches (i.e., those poor in amylose or highly processed) can have a higher GI than sugars (e.g., fructose and lactose). For example freshly boiled white rice and potato have GI values of 89 and 98%, respectively (Atkinson et al. 2008) with an II as elevated as 79 and 121 (Holt et al. 1997).
There is adequate evidence from cohort studies that higher consumption of dietary fiber is associated with reduced risk of T2D (SACN 2015). As non-digestible moieties, dietary fiber have a GI of 0, and thus their intake does not contribute to postprandial glycemia and insulinemia. In addition, some viscous fibers such as ß-glucan, pectin, guar gum or glucomannan, when incorporated into high glycemic foods, have the capacity to lower the glycemic and insulinemic responses (Jenkins et al. 1986).
High GI and GL foods
The plausibility of causality behind the association between some carbohydrates or carbohydrate-rich foods and T2D can be reinforced by the analysis of cohort and clinical studies examining the impact of the intake of low vs high GI foods.
According to the SACN report (2015), the analysis of prospective cohort studies shows that a diet higher in GI or GL is associated with a greater risk of T2D. Interestingly, sugars sweetened beverages which are positively associated with T2D (DGAC 2015 SACN 2015) have a GI ranging from moderate to high (i.e, 40 to 78), the highest being sport drinks, and have a GL higher than 10.
However, randomized controlled trials have not provided consistent evidence of an effect of GI or GL on surrogate markers or risk factors of T2D such as fasting blood glucose
and insulin (SACN 2015). The heterogeneity of the macronutrient composition of the tested low vs high GI/GL diets may explain this inconsistency. In addition, most studies have not measured the GR and when they have been measured they do not always achieve meaningful blood glucose differences (Blaak et al. 2012). Therefore, the use of more direct measures of glucose and insulin postprandial exposure than GI/GL and II,
such as for instance continuous glucose monitoring or urine cpeptide, are needed to better define a healthful digestible/glycemic
carbohydrate intake.
Key messages
–Greater intake of free/added sugars is associated with higher risk of T2D, particularly when consumed as sugars sweetened beverages.
–Not all sugars have the same GI and II. Some complex carbohydrates (e.g., maltodextrins, refined & highly processed starches) have higher GI and II than sugars (e.g., lactose, fructose, isomaltulose)
–Diet higher in GI or GL is associated with a greater risk of T2D but the evidence based on randomized control trials is not consistent
–Intake of dietary fibers is associated with reduced risk of T2D
–Some soluble viscous fibers lower the glycemic and insulinemic response of foods
Cardiovascular diseases
CVD are a group of disorders related to the heart and blood vessels. Myocardial infarction and cerebrovascular accident,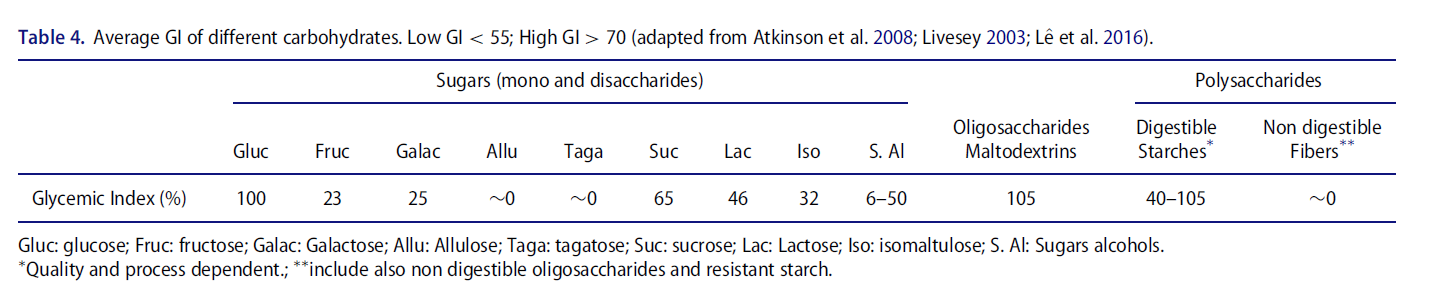
which are the acute and often fatal phases of the diseases, are due to the blockage by atherosclerotic lesions of the blood, from flowing to the heart or brain (WHO 2016). The combination of high levels of LDL cholesterol and triglycerides (hyperlipidemia) accelerates atherosclerosis increasing the risk of heart attack and stroke. Diabetes is also a prime risk factor for CVD since chronic high blood glucose levels promote macro
and micro-vascular damage.
Other risk factors include tobacco use, excessive consumption of alcohol, unhealthy diet, obesity, hypertension, fatty liver and physical inactivity (World Heart Federation 2016). Therefore, as CVD have multifactorial causes, it is difficult to point out one specific property linking sugars/carbohydrates to their development. However, a simplified view may be that their main direct effects rely in their ability to modulate lipid homeostasis.
Sugars
According to the SACN report (2015), there is insufficient evidence from cohort or randomized controlled studies to conclude on the impact of high sugars intake and CVD risks. However, the limited evidence tends to favor a positive association. Indeed, a recent study of a prospective cohort in the US, showed a significant relationship between added sugars consumption and increased risk for CVD mortality (Yang et al. 2014). In addition, a meta-analysis of randomized controlled trials concluded that greater intake of sugars (especially sucrose or high-fructose corn syrup) raises blood pressure, cholesterol and triglycerides (independently of body weight) (Te Morenga et al. 2014). With respect to the DGAC, their report concludes on a moderate evidence that higher intake of added sugars, especially as beverages, is associated with CVD (DGAC 2015).
They also found a consistent relationship between higher consumption of added sugars and increased blood pressure and triglycerides.
Among the different sugars, fructose, either alone or as a component of sucrose or high-fructose corn syrup, seems to be the most detrimental to metabolic and cardiovascular health. Indeed, when ingested in excessive amounts (>50 g/day) and compared to the same amount of glucose, fructose has been shown to increase blood postprandial triglycerides (Livesay and Taylor 2008) and LDL-cholesterol (Stanhope et al. 2011). It
also promotes the accumulation of fat in the liver increasing the risk of developing hepatic insulin resistance as well as nonalcoholic liver steatosis (Faeh et al. 2005; L^e et al. 2009). A intake of one liter of a sweetened beverage could lead to a consumption
of 60 g fructose, while providing an additional 60 g of glucose.
Oligo- and polysaccharides
There is a lack of available evidence on the potential association of starch or starchy foods intake with CVD. On the other hand, observational studies have shown inverse associations between high intake of dietary fibers and cardiovascular diseases, coronary
events and stroke. When the type or origin of the dietary fiber was analyzed, insoluble fiber, vegetable and cereal fibers were, or tended to be, protective against cardiovascular diseases and coronary events (SACN 2015).
Randomized controlled trials show that higher intake of the soluble fiber beta-glucans and one of their main natural source, oat bran, promotes a reduction of several CVD risk factors, including blood LDL cholesterol, triglycerides and blood pressure
(SACN 2015).
High GI and GL foods
Prospective cohort studies indicate that there is a relationship between high GL, but not GI, diet and increased risk of CVD. Based on randomized controlled trials, a low vs high GL diet might promote a reduction of blood pressure and serum triglycerides
(SACN 2015). Nevertheless, the evidence regarding GI/GL foods and CVD remains very limited.
Key messages
– Greater intake of free/added sugars might be associated with higher risk of CVD, probably through an increase in blood pressure and triglyceride levels
–Fructose seems to be the main sugar associated with the increased CVD risk
–An excessive daily fructose intake is not readily achievable by consuming whole fruits but can be easily reached with fructose/sucrose rich beverages.
–Elevated postprandial glycemic and/or insulinemic responses might contribute in increasing CVD risk, but more evidence is needed to confirm this hypothesis.
–Higher intake of different types of dietary fibers is inversely associated with cardio-vascular and coronary diseases.
–Intake of viscous soluble fibers, such as beta-glucans, decrease CVD risk factors
Conclusions
The current scientific evidence regarding the role of dietary carbohydrates on health and diseases tends to allow the distinction between two categories of carbohydrates:
(1) “The healthful”, composed of no/low cariogenic and/or non/slowly-digestible carbohydrates, such as slowly digestible starch, dietary fibers, lactose, isomaltulose or
tagatose.
(2) “The health sensitive”, consisted of cariogenic, high GI or dyslipidemic carbohydrates, such as fructose, glucose, sucrose, maltodextrins and rapidly digested starch. In order to improve the nutritional value of food products, formulation of carbohydrate blends specific and adapted to different food matrices need to be explored. The utilization of the healthful carbohydrates at the expense of the health sensitive ones should be favoured. The main challenge is to find, in different food matrices, the right ratio between these 2 categories of carbohydrates, taking into account the nutritional needs of the individual and product application (e.g., general population, sport or clinical nutrition), as well as the physiological impact and limitations in terms of safety/tolerability, production and organoleptic properties. Given that the average intake of dietary fiber in most Western countries is only half of the recommended levels, it is imperative that this challenge is addressed. Although recommendations differ, the recommended fiber intake for adults usually ranges from 25–38 g/d (EFSA 2010, IOM 2005, SACN 2015).
The healthful carbohydrates listed above are commercially available as ingredients that have been isolated from their natural sources. However, the components of whole foods that constitute healthful carbohydrates, are considered as such because they also provide phytochemicals, vitamins and minerals. The following section highlights the main types of healthful carbohydrates those which should be consumed as part of a healthy
diet and thus should be favoured in the development of food products with a healthier carbohydrate profile. Furthermore, an important component of food product development that is often overlooked is food processing. As in the nutrition field, research in food science is evolving constantly and the impact of processing on the organoleptic properties of food has been extensively characterized. Here, we also highlight the importance of studying the impact of food processing on the nutritional properties of food products as well as discuss its potential on preserving and potentiating the nutritional value of healthful carbohydrate sources.
Types of healthful carbohydrates and their sources
Carbohydrates comprise a wide range of saccharides and current nutritional recommendations are based on their classical chemical classification; simple carbohydrates are constituted by mono- and disaccharides commonly referred to as sugars, and complex carbohydrates includes all the rest, oligo- and polysaccharides
(Table 1). However, this chemical classification does not always translate equally when evaluating their nutritional quality. In fact, emerging research has shown that both healthful and “health sensitive” (when consumed in excess) carbohydrates can be found within the same group of chemical classification. For instance, the soluble fiber β-glucan, which is known for its health benefitting property, is categorized as a polysaccharide based on its chain length. In the same group, maltodextrins derived from starch can also be found if their dextrose equivalent (DE) value is low enough to be classified as polysaccharides. The following subsections describe the specific types of carbohydrates considered healthful based on the ways in which they are metabolized and not on their chemical classification.
Dietary fibers
EFSA (2010) defines dietary fibers as carbohydrates plus lignin, including all carbohydrate components occurring in foods that are non-digestible in the human small intestine and pass into the large intestine. In addition, the CODEX definition specifically refers to carbohydrate polymers of 10 or more monomeric units and states that dietary fiber is constituted by a) edible carbohydrate polymers naturally occurring in the food as consumed (e.g. whole grain), b) carbohydrate polymers obtained from food raw material by physical, enzymatic, or chemical means (e.g. fructooligosaccharide), and c) synthetic
carbohydrate polymers (e.g. polydextrose). Furthermore, carbohydrates that fall into categories b and/or c, must show a proven physiological benefit to health as demonstrated by generally accepted scientific evidence to competent authorities before they can be labelled as dietary fibers. Therefore, dietary fiber includes a wide range of carbohydrates such as nondigestible oligosaccharides (NDOs), non-starch polysaccharides (NSPs, such as pectins, and ß-glucans), hydrocolloids such as mucilage, and resistant starches. To further illustrate the complexity of dietary fibers, in the case of resistant starches (RS) there are 4 types, namely, RS1, RS2, RS3 and RS4. RS1 refers to the portion of starch naturally found in raw/unprocessed seeds, legumes, or whole cereal grains that is resistant to digestion, and RS2, in grain mutants that have been bred to produce starches with a particular structural conformation that is resistant
to digestive enzymes. RS3, on the other hand, is produced in cooked and cooled starchy foods where the starch has recrystallized or retrograded (i.e., stale bread and cold potato salad). Finally, the RS4 is constituted by chemically modified starches that resist digestion. Furthermore, non-starch polysaccharides in cell wall tissues are usually found intricately entangled with lignin, which is not a carbohydrate but a phenolic polymer, and
is therefore considered a component of dietary fiber. As can be deduced from the examples provided, dietary fibers, natural or synthetic, are predominantly of plant origin.
Cereal grains, pseudocereals and pulses, which are important components of the diet, are good sources of dietary fiber (Table 5). The majority of the dietary fiber from these sources is insoluble because the dietary fiber is mainly concentrated in outer layers, bran and hulls, of the grain or seed. In addition,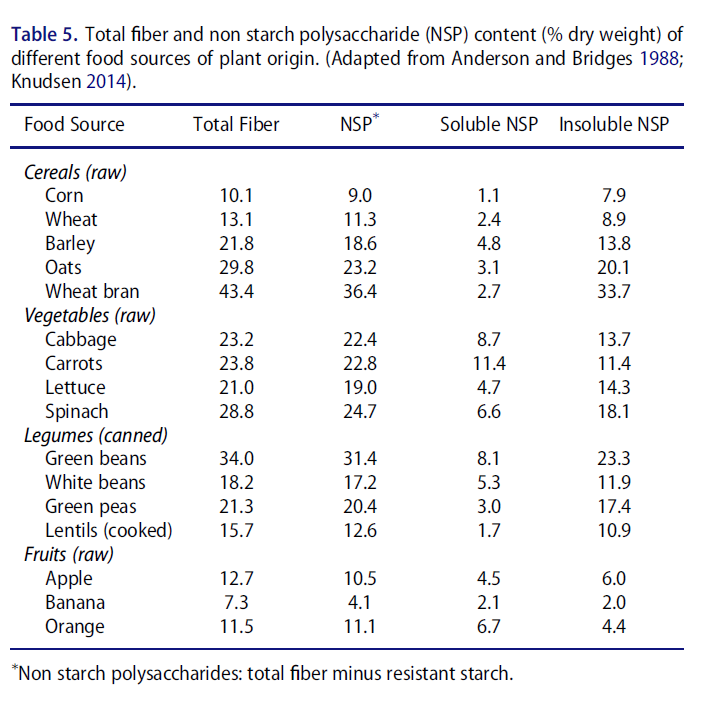
resistant starches (RS) are usually insoluble due to their structural conformation and large molecular weight. Different physiological effects have been attributed to insoluble (e.g. improve laxation) and soluble dietary fiber (e.g. lowering of blood cholesterol
or glucose) however, this difference of solubility does not systematically predict physiological effects. Among the natural sources of fibers, cereal fibers have been more strongly associated with a reduction of T2D than fibers from fruits and vegetables (Lê et al. 2016). Interestingly, the interaction between dietary fiber and the gut microbiome is an emerging mechanism to explain the positive association between dietary fiber intake and cardiometabolic health. However, more research is needed to demonstrate causality and identify the most beneficial fiber and gut microbial composition.
Slowly digestible carbohydrates
Starch is a major source of energy in the human diet and its specific macro and fine-structural features, such as crystallinity or amylose:amylopectin ratio, largely determine its susceptibility to digestion in the small intestine (Behall et al. 1988; Zhang and Hamaker 2009). Starches that have higher proportions of amylose have slower digestion rates and/or are more resistant to digestion (Jane et al. 1999; Chung et al. 2011). In order to differentiate the digestive properties of starches in foods, a classification into rapidly digested starch (RDS), slowly digested starch (SDS) and resistant starch (RS), the latter being classified as a dietary fiber, was proposed by Englyst et al. (1996). Most
raw cereal, pulse and tuber starches contain considerable amounts of both SDS and RS. Table 6 shows the content of these three types of starch in different food sources. The nutritional relevance of SDS is based on its slow rate of digestion, which in turn, elicits a lower, plateaued GR (Ells et al. 2005). When applied to food manufacturing, this results in products with lower GI values (Goñi and Valentín-Gamazo 2003). The quantification of RDS, SDS, and RS is the result of the Englyst in vitro digestibility analysis that is based on simulating the action of digestive enzymes on starch or starchy food samples analyzed ‘as eaten’. Thus, it is important to note that the levels of RDS, SDS and RS may vary for each food source depending on the specifics of the cooking method (temperature, pressure, moisture content, pH, etc.) used (Bravo et al. 1998, Mishra et al. 2008). Furthermore, subsequent storage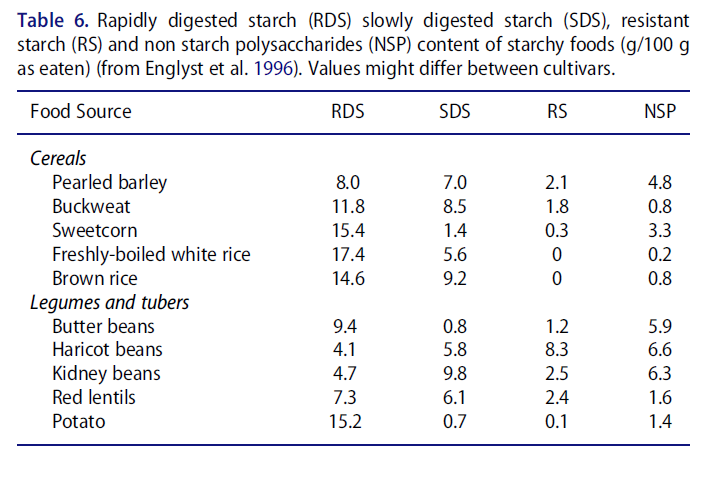
conditions of cooked starchy foods have a direct impact on the amount of SDS that the food contains. For instance, Monro et al. (2009) have shown that cooling freshly cooked potatoes result in significantly greater amounts of SDS in particular genotypes.
Other than slowly digestible starches, sugars with slowly digestible properties also exist. Isomaltulose is a slowly-digestible disaccharide (Holub et al. 2010) composed of glucose and fructose linked by an (α1→ 6)-glycosidic linkage that naturally occurs in honey and sugar cane extract in very small quantities (Low and Sporns 1988). It is available as a commercial ingredient produced by the enzymatic isomerization of sucrose (Mu
et al. 2014). It has about 50% the sweetness of sucrose and its expected physiological response is similar to that of SDS but their techno-functional properties differ greatly. Indeed, studies of its digestibility in vitro have shown that its rate of hydrolysis
is significantly slower than that of sucrose and maltose (Tsuji et al. 1986). In agreement, clinical studies have shown that the postprandial glycemic and insulinemic responses to isomaltulose rise at a slower rate, and maximum concentrations reached are lower than sucrose (Maresch et al. 2017).
Lactose is another disaccharide that has a low GI (Table 3), which is attributed, in part, to a slow rate of hydrolysis of its components, glucose and galactose and to the low GI of galactose itself (Gray and Santiago 1966; Rerat et al. 1984). Milk is the highest food source of lactose (about 5 to 7% in bovine and human milk, respectively) and also provides proteins, vitamins and minerals, especially calcium.
Low calorie sugars
Low calorie sugars represent interesting candidates for sucrose replacement. There exists more than 30 mono- and disaccharides, among which 24 have a caloric content lower than 4 kcal/g (Vafeiadi et al. 2015). The method to establish available energy for such sugars yield different results from those obtained by the traditional bomb calorimeter. Indeed, the principle of the latter rests on the energy released by complete combustion of the molecules. In this case, all carbohydrates have an energy content similar to that of glucose, i.e. around 4 kcal/g (Livesey 1990). In contrast, available energy relies on the amount of energy that is available for cell metabolism. In vivo, this can be measured by a combination of tracers and indirect calorimetry methods. Only few studies have investigated the effect of low caloric sugars in humans, and most studies refer to tolerance/digestive comfort. To our knowledge, only arabinose, xylose, tagatose and allulose have been studied in humans for metabolic outcomes. Today, tagatose and allulose are the two low caloric sugars with the highest potential for sugar replacement,
as the technical developments to incorporate them into food products are the most advanced and both have been granted a GRAS status by the US FDA.
Both tagatose and allulose are naturally found in some foodstuffs (Oshima et al. 2006, Levin 2002), such as dairy products and cereals, albeit in very small quantities. Ingredient suppliers are currently developing biotransformation processes for their industrial production. Tagatose is manufactured from galactose through enzymatic and chemical processes (Oh 2007), while allulose is produced at an industrial scale by the enzymatic isomerization of fructose (Takeshita et al. 2000). These sugars have similar physicochemical properties as sucrose, glucose or fructose, therefore they can be easily used to replace sugars. Their main difference lie in their absorption and metabolism.
Tagatose has an available energy content between 07–1.5 kcal/g (Levin et al. 1995). Its low caloric content is mostly due to its incomplete intestinal absorption. Rats studies
have shown that only 15–20% of ingested tagatose was absorbed (Levin 2002), which at doses above 30 g can yield intestinal discomfort in humans. For metabolic health, it has
been shown that moderate doses of tagatose (5–10 g) decreased glucose-induced postprandial glucose and insulinemic reponses Kwak et al. 2013). The mechanism involved is not clearly understood. In addition to the GRAS status by the US, tagatose
has an EFSA-approved health claim for tooth demineralization and lower glucose response (EFSA 2011).
Allulose has an available energy content of 0.2 kcal/g. In contrast to tagatose, after oral administration, ≈70% of allulose is absorbed and excreted via urine. This suggests that the absorbed allulose is not or minimally metabolized. The proportion of allulose that is unabsorbed may pass through the colon and be fermented by gut bacteria (Hossain et al. 2015). Oral administration of allulose decreases maltodextrin-induced glucose
excursion, both in healthy subjects and in subjects with impaired glucose tolerance (Hayashi et al. 2010). The postulated mechanism may involve inhibition of a-glucosidases (Hayashi et al. 2010). Despite these promising effects, some early toxicity studies in rats showed increased liver and kidney weight, which warrants caution and further investigations to determine chronic effects in humans (Matsuo et al. 2003, 2012)
In summary, a healthful carbohydrate profile is constituted by dietary fibers, slowly digestible carbohydrates and, when a certain level of sweetness is required for palatability, low amounts of sugars, preferably those of low-caloric value. Opting for the consumption of cereal grains, pulses, fruits and vegetables in their whole form will significantly contribute to the intake of healthful carbohydrates. These sources should contribute to a healthy diet and should be preferred for the development of food products with “blends of healthful carbohydrates” as previously described. However, the recalcitrant nature of insoluble dietary fibers present in whole foods and the susceptibility of raw starch crystallinity to cooking pose considerable technological challenges.
Processing healthful carbohydrates: Current challenges and opportunities
Historically, humans have employed a variety of cooking techniques in order to improve the organoleptic and nutritional quality of food (e.g., increased food digestibility) (Carmody et al. 2011). Although industrial food processing generally tends to be negatively perceived by the general population (Cardello 2003), it is often key for preservation by achieving reductions of anti-nutritional factors (Hotz and Gibson 2007),
toxins, or pathogenic microorganisms (Beuchat 2002). The knowledge in the field of food processing is vast and each type of macronutrient imparts specific changes to foods during processing. Here, we focus on examples of food processing techniques that are relevant for sources of healthful carbohydrates.
As in traditional cooking settings where for instance fruits are peeled or grains are dehulled, sources of healthful complex carbohydrates (e.g., whole grain) are often refined to circumvent the technological challenges, poor organoleptic quality and consumer acceptance of the final products (Poutanen et al. 2014). Nonetheless, healthful carbohydrates can be incorporated into food products with minimal impact on the organoleptic properties of food products and potentially improved nutritional value with the aid of processing. Carefully selected or designed food processing techniques can effect changes on the physicochemical characteristics of healthful carbohydrates, which may allow for their incorporation into food at nutritionally relevant quantities (Wen et al. 2017 Agama-Acevedo et al. 2016). However, when sources of healthful carbohydrates are processed as part of a recipe, the impact on the other ingredients must be considered as well. It is well known that processes of high heat, moisture and shear conditions convert raw starch into a rapidly digestible nutrient that triggers an elevated glycemic and insulinemic responses, when consumed (van
Amelsvoort and Weststrate 1989 Wang and Copeland 2013). Therefore, the specific changes to physicochemical properties of nutrients in foods should be carefully considered when investigating their physiological impact. The processing technologies that are widely used for sources of healthful carbohydrates include mechanical fractionation or milling, thermal treatment or cooking, extrusion and enzymatic hydrolysis.
Mechanical fractionation or milling
Dehulling has been traditionally used in households to remove the tough outer layers of cereal grains in order to improve their palatability and for the removal of anti-nutritional factors. Mechanical fraction or milling of cereal grains is the process by which flours are produced at a larger scale. It may be considered the industrial equivalent of dehulling because the production of refined or “white” flours consists of removing the bran and germ to isolate the starchy endosperm of the grain. The removal of such grain components produces flours that are more stable upon storage, have improved processability, and result in food products of preferred sensory quality (i.e., white bread versus whole grain bread). However, refined flours have a total dietary fiber content that is about four times less than that of whole grain flours (Slavin et al. 2000) and, thus, refined cereal flours lack other nutritionally relevant compounds that are found in the bran and germ components (Hemery et al. 2007). Due to the impact that bran and germ components have on stability and sensory quality of whole grain food products (i. e., rancidity, rough textures and darker colors), substantial research efforts have focused on understanding how to process whole grains to enhance their consumption (Slavin and Lloyd 2012). Currently, the recombination of individual whole grain constituents obtained via traditional milling is a widely used and accepted practice for the preparation of whole grain flours and products (van der Kamp et al. 2014, Ross et al. 2017). Similarly, fruits and vegetables are largely consumed without their peels, which are usually inedible, and this practice results in a 50% decrease of their dietary fiber content. Herein lies the main difference in consuming fruit purees, juices, and/or concentrates instead of whole fruit. However, the nutritional value contained in the peels can be salvaged via various processing technologies. In fact, the extraction of dietary fibers such as pectins, which have been shown to have beneficial health effects, is aided by the mechanical fractionation of discarded peels from citric fruits and apples. Powders manufactured from
fruit peels can also be used as ingredients for fiber fortification in a variety of food products (Figuerola et al. 2005, Ajila et al. 2008).
Thermal treatment
Thermal treatment or cooking is the main form of food processing carried out in households and is equally prevalent in the food industry. Cooking by heat application to
raw foodstuffs generates the desired flavors and textures as well as ensure that they are safe for consumption. Heat treatment of native starch (as found in raw tubers, cereals
and pulses) in the presence of water, such as boiling potatoes or baking bread, results in the loss of the starch granular structure and its subsequent gelatinization. Gelatinized
starch is considerably more susceptible to digestive enzymes (Holm et al. 1988, Hernot et al. 2008). Factors such as concentration, fine structure, presence of dietary fibers and the food matrix in which it is embedded have an influence on the extent of starch gelatinization (Lovegrove et al. 2015). Conversely, thermal treatment can also be used to reduce the susceptibility of starch to digestion. Annealing of starch is a type of heat treatment with specific temperature and moisture conditions that alter the crystallinity of starch granules and stabilize their native structure (Tester and Debon 2000). Additionally, when thermal treatment is followed by cooling cycles, the gelatinized starch undergoes a
second structural transformation, referred to as retrogradation, that renders the starch more resistant to digestion (Ottenhof and Farhat 2004). For example, the starch in
boiled potatoes undergoes retrogradation when the potatoes are stored at refrigeration temperatures overnight (Nayak et al. 2014). Thus, the processing of starchy-foods should target a balance between preserving or effecting slow-digestion profiles as well as preferred organoleptic properties.
Besides starch, thermal treatment can also impact nonstarch polysaccharides. The preparation of oat porridge, for instance, solubilizes beta-glucans contained in the oat flakes. For this reason, it is important to realize that viscous and soluble dietary fibers such as beta-glucans or pectins, which bear approved health claims related to cholesterol and blood glucose, are sensitive to heat and shear. Indeed, when pectin and
beta-glucans are heated or exposed to shear they tend to depolymerize and such changes can impact the health benefits they confer (Regand et al. 2009; Gunness and Gidley 2010). Nonstarch polysaccharides in their insoluble form are also changed by thermal treatment. Cereal brans, which are predominantly insoluble and used for animal feed, undergo a certain level of solubilization when subjected to high heat and pressure conditions (Rose and Inglett 2010). Through targeted processing, cereal brans can be a source of soluble fibers or prebiotic oligosaccharides.
Finally, thermal treatment is applied extensively for drying purposes. Although this tends to be the final step in a processing line, its effects on carbohydrate physicochemical structures should not be overlooked. Depending on the conditions, drying has been shown to change the molecular and digestibility properties of flours in products such as pasta (Stuknyte et al. 2014). Different types of drying processes can also impact the functionality of carbohydrates by changing their hydration capacities and texture properties (Mandge et al. 2014).
Baking
Baking is another type of thermal treatment that is extensively used in the processing of many cereal-based products such as breads and biscuits. However, the effects of baking on the nutritional value of baked goods is largely dependent on the recipe (i. e. water, proteins and fiber content) (Garsetti et al. 2005). The “gentle” form of heat application that occurs during baking does not always effect a dramatic change to the native starch and, if designed purposefully, can actually result in products composed of cereal starches that have a reduced rate or degree of digestibility (Lehmann and Robin 2007). In addition, resistant starch can be generated during the baking and subsequent cooling processes (Sanchez-Pardo et al. 2007, Hallstrom et al. 2011).
Extrusion
Food extrusion is a process where a combination of raw materials is forced through a screw under different conditions of heat, moisture, pressure and mechanical shear (Alam et al. 2016). The impact of extrusion on carbohydrates depends on the specific conditions and the physicochemical features of the ingredients used. The combination of heat, pressure and shear during extrusion can result in the complete or partial gelatinization of starch, or on the generation of resistant starches when other processing aids such as organic acids are used (Hasjim and Jane 2009). Similar to the effects of thermal treatment, non-starch polysaccharides also undergo depolymerization during extrusion (Hernot et al. 2008; Yan et al. 2015). Specific modulation of extrusion parameters in combination with tailored formulations can improve the organoleptic properties of starch and dietary fiber blends (Redgwell et al. 2011). For example, it was reported that the expansion properties of extruded wheat flour was impacted by the addition of wheat bran due to an increase in melt viscosity (Robin et al. 2011). Altan et al.(2009) have also shown that the incorporation of fruit pomace in extruded blends of cereal flours resulted in lower digestibility of starch. Thus, the optimization of extrusion parameters and product recipes is of interest for the generation of carbohydrate blends with acceptable organoleptic properties while maintaining or improving the nutritional value of the carbohydrates.
Enzymatic treatment
Common examples of the application of enzymatic treatment in food processing is the baking of yeast-leavened and sourdough breads (Linko et al. 1997) and the production of alcoholic beverages (Bamforth 2009). The food industry applies enzymatic treatment in a variety of ways. For instance, one of the ways to produce common food ingredients such as maltodextrins and glucose syrups is via enzymatic hydrolysis of starch (Guzman-Maldonado and Paredes-Lopez 1995). Another example is the hydrolysis of complex carbohydrates for ease of processing because large polymers generate highly
viscous pastes that are difficult to pump. As previously discussed, changes to the physicochemical properties of native starches have a direct impact on their digestibility, and hydrolysis of the high molecular weight, starch structure into low molecular weight polymers significantly increases the rate at which it is digested. On the other hand, emerging research has shown the potential of using enzymatic treatment to reduce the
digestibility of processed starches (Wu et al. 2015). The generation of highly-branched starch hydrolyzates have been shown to have a comparably slower digesting property both in vitro and in vivo (Lee et al. 2013), however, further research on how these enzymatically branched starches behave in food products is required.
As previously mentioned, isomaltulose, a slowly digestible disaccharide is produced by the enzymatic isomerization of sucrose. Sucrose can also be enzymatically converted into fructooligosaccharide (FOS), a non-digestible oligosaccharide, by means of fructosyl transferases (Singh et al. 2010). These particular enzymatic reactions convert a rapidly-digested disaccharide into a slowly-digested disaccharide or an indigestible oligosaccharide that does not elicit a high GR. Such enzymatic transformations occur in nature for different purposes and their large-scale application in the food industry can be an opportunity for the development of healthful carbohydrate blends.
In the case of dietary fibers, enzymatic treatments are predominantly used to solubilize fiber components from biomass or cell wall material in order to potentiate the value of plant material that is traditionally discarded. Isolated fiber ingredients have lower impact on the organoleptic properties of food products they are used in. FOS can also be produced from the enzymatic hydrolysis of inulin, which is a fructan polymer of
longer chain length. Thus, enzymatic treatment of carbohydrates, in some cases, can be beneficial by changing structural features that result in carbohydrates of low GR or that allow for the enrichment of fiber in food products. A balance between ease of processing and nutritional/physiological values should be always considered.
Conclusions
The impact of food processing on the physicochemical properties of carbohydrates is very complex and, contrary to popular belief, it can contribute significantly to the consumption of healthful carbohydrates by providing means to create them during the manufacture of the product. More specifically, the selection of carbohydrates sources can be tailored to the type of process and vice versa. The optimal combinations can only be possible if the changes that healthful carbohydrates undergo during processing are properly assessed. Such changes should be analyzed in terms of nutritional value but also organoleptic properties because a carbohydrate blend with good nutritional
quality can only be healthful if consumed. Therefore, to have a better understanding of how to design or choose the best carbohydrate sources and processing parameters to create healthful carbohydrate blends, the physiological responses elicited should be evaluated in parallel to the impact of such factors on the organoleptic properties of food product, while preserving or increasing nutritional quality as much as possible.
Proposals for future developments
Current knowledge, and evidence linking carbohydrate quality to health, provides scientific support for a number of future developments, including avenues for future research as well as projects linked to product development.
1. This paper provides the rationale for not simply classifying carbohydrates based only on their chemical basis. Carbohydrates should also be classified according to
their physiological impact since not all sugars are detrimental to health and not all complex carbohydrates are neutral. Indeed, from a health perspective current dietary recommendations for sugars should be based on their functional properties and physiological effects and not simply on their chemical classifications. For these reasons,
well-characterized sugars with both no/low cariogenicity, low GI and lipogenic capacity (i.e., lactose, isomaltulose, tagatose and allulose) might be considered differently regarding the “free/added sugars” labeling as done for sugar alcohols. By contrast, dietary recommendations to prevent excess intake could be extended to oligo- and polysaccharides with potential cariogenic properties and/or promoting a high glycemic and insulin response.
2. Further work on the role of sweet taste perception and exposure on eating behaviour and energy intake could help to identify the drivers of over-consumption of sweet foods, especially sweet energy dense foods.
3. Further research is needed to demonstrate the underlying mechanisms linking postprandial glycemia to cardiometabolic disorders and to identify very early predictive
risk biomarkers.
4. This review has also highlighted the need for relevant reformulation of manufactured foods. This includes the three following activities:
a. Firstly, studying and developing healthful carbohydrate blends that will contribute to the effort of improving consumers’ diets.
b. Secondly, characterizing the physico-chemical properties of alternative carbohydrate sources (e. g., cereal brans, pulses and/or legumes) or their isolated fractions (e. g., soluble fibers and resistant starches) in order to develop optimized blends that have improved ratios between glycemic and non-glycemic carbohydrates. This would also need to take account of nutritional needs, tolerance as well as technological and taste limitations.
c. Thirdly, studying the impact that structural features (chain length, type and frequency of branches) of glycemic carbohydrates have on their rate of digestibility.
5. The impact of product formulations and industrial processing technologies on energy intake and postprandial glycemic/ insulinemic and lipid responses is not fully understood, and so further research would be useful.
6. Finally, this review supports the case for developing evidence- based and consumer-friendly communication to guide consumers towards healthier manufactured food
and beverage products.
Lamothe LM. Et al. The scientific basis for healthful carbohydrate profile. Critical Reviews in Food Science and Nutrition 2019, VOL. 59, NO. 7, 1058–1070