Nutritional Approaches for Weight Management, and Prevention and Remission of Type 2 Diabetes
INTRODUCTION
Obesity is traditionally measured by BMI;1 however, more recent studies point to how adverse outcomes associated with being overweight, such as cardiovascular disease (CVD) and T2D, may be more associated with VIF accumulation and distribution.2,3 As such, dietary programs may need to assess not only simple weight loss, but how they affect body fat distribution.
At the ADA 81st Scientific Session, 2021, held virtually, a symposium was presented by Neeland and Taylor that highlighted the role of VIF in the pathogenesis of obesity and T2D along with weight management programmes that can help target VIF.
Visceral Fat and its Role in the Pathogenesis of Obesity and Comorbidities - Ian J Neeland
Visceral and Ectopic Fat Versus BMI
Currently, approximately 40% of the adult population in the USA are considered obese.4 This is of concern as obesity is associated with lifetime incidence of CVD morbidity and mortality.5 The traditional way to identify at-risk adults has been via calculation of BMI;1 however, according to Neeland: “We know that the BMI–health outcomes relationship is heterogenous. Many patients with obesity never develop CVD or metabolic diseases, whereas others who are not obese will.”
Neeland suggested that one of the most important aspects in determining such disease risk was actually variation in VIF burden. By illustration, he presented the case of a mildly overweight (BMI: 26 kg/m2) 43-year-old male with average low-density lipoprotein (LDL) cholesterol (116 mg/dL) and blood pressure (135/65 mmHg). Body fat analysis via MRI and advanced lipid analysis revealed that his visceral adipose tissue was at the 95th percentile for his age/BMI6 his liver fat fraction was 25% (upper normal range: <5.5%);7 his HbA1c was 6.0% (pre-diabetes: 5.7−6.5%);8 he had an increased concentration of small LDL particles associated with atherogenic dyslipidaemia9 and elevated triglycerides of 240 mg/dL (reference: <150).9 Despite being classed as only mildly overweight, these figures, Neeland explained, meant this male had an elevated CVD and T2D risk and was a classic case of someone who was “obese on the inside” (Figure 1).
What potentially underlies this is dysfunctional adiposity, which, according to Neeland, is “a pathologic response by adipose tissue to positive caloric balance in susceptible individuals that directly and indirectly contributes to cardiovascular and metabolic disease.” Dysfunctional adiposity is characterised by excess VIF deposition, inflammatory and adipokine dysregulation, insulin resistance, and atherogenic dyslipidaemia.2 This, said Neeland, “makes VIF a very attractive, modifiable target to track weight loss outcomes.”3
Ectopic fat accumulation starts when an imbalance between caloric intake and/or energy expenditure leads to a positive energy balance. Increased triglycerides deposited in adipose tissue can cause inflammation and, when adipose tissue can no longer expand, a spill-over of excess lipids into tissues that don’t usually contain them, such as the liver, pancreas, muscles, and heart. This, explained Neeland, can create inflammation and insulin resistance that can lead to adverse cardiometabolic outcomes.2

Figure 1: Extreme variation in abdominal fat distribution.
T1-weighted coronal neck-to-knee MRI images demonstrating variation in abdominal subcutaneous fat (blue) and visceral fat (red) between an individual with normal weight but high visceral fat (left) and an individual with obesity but lower visceral fat (right).
Images courtesy of AMRA Medical (Linköping, Sweden). Adapted from Neeland et al.3
Indeed, in an investigation utilising data from the Dallas Heart Study, the risk factor most strongly predictive of T2D was visceral fat mass (odds ratio [OR]: 2.4; 1.6–3.7), with lower ORs for fasting glucose (OR: 1.9; 1.4–2.6), weight gain (OR: 1.3; 1.1–1.2), and systolic blood pressure (OR:1.3; 1.1–1.5).2 Another study showed that with increasing quartiles of visceral adipose tissue came increasing incidence of CVD (hazard ratio:1.21; 1.02–1.43).10
Interventions Targeting Visceral Obesity
Interventions for visceral obesity include nonpharmaceutical, pharmacological, and surgical approaches, and, Neeland highlighted, choice might depend on “the treatment intensity needed, the presence or absence of current disease, and whether or not the previous modality worked” (Figure 2). He further stressed that they fundamental treatment for weight loss, as well as for VIF, stems from lifestyle interventions. Current USA weight management guidelines suggest a caloric-based dietary plan with an initial prescription of 1,200−1,500 kcal/day for females and 1,500−1,800 kcal/day for males, representing a 500−700 kcal/day energy deficit.12 A calorie-restricted diet can be based on patient preference, food types, and health status but the Mediterranean Diet is the diet with the most consistent and robust scientific support in reducing atherosclerotic CVD risk12 and the diet most suggested by Neeland to his patients to both lose weight and improve cardiovascular risk.
That lifestyle modification reduces VIF was illustrated by a study where 278 adults with obesity and/or dyslipidaemia were taught a multiple-daily lifestyle intervention that included either a low-fat or a Mediterranean/lowcarbohydrate diet, with or without increased physical activity. After 18 months, the dietary modification cohort, regardless of physical activity, improved with regards to weight and waist circumference.13
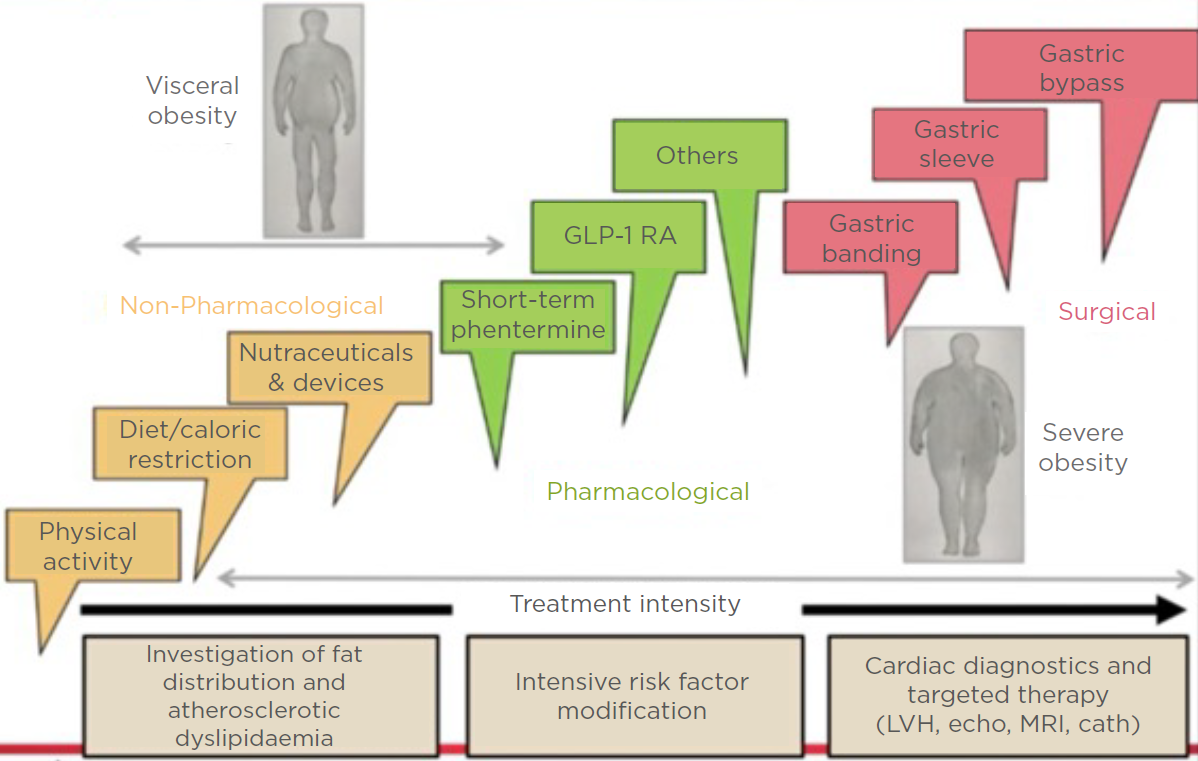
Figure 2: Interventions for (visceral) obesity.
Cath: cardiac catheterisation; echo: echocardiogram; GLP-1 RA: glucagon-like peptide 1 receptor agonists; LVH: left ventricular hypertrophy.
Adapted from Despres et al.11
Although the degree of weight loss wasn’t high (around 5% overall), pre- and post-imaging of VIF depots revealed that degree of fat decrease over time was much greater than weight change. Liver fat, for instance, went from 28% to 5%, which was, explained Neeland, “a much greater fold decrease than one would expect if just monitoring weight loss and waist circumference.” What this showed, he continued, was that “even if the patient may not be losing generalised body weight…keep in mind that the VIF may be modified significantly, which has long-term beneficial outcomes.”13
Very Low Energy Diets
Myriad diets create confusion regarding what’s best, reported Neeland, with the ketogenic diet being the one he is asked about most. This is a restricted-carbohydrate, high-fat diet where the goal is 90% long- or medium-chain triglycerides in a 4:1 lipid to non-lipid ratio. Compared with usual care, one study showed that a ketogenic diet could significantly decrease several cardiometabolic risk factors, weight and lipid measurements, and improve glucose tolerance.14 However, Neeland posited that the success of this low-carbohydrate diet might actually be due to it being calorie restrictive. This is illustrated by a study that compared high- versus lowcarbohydrate diets and found that the latter was approximately 500 kcal/day less. Weight loss was associated with longer diet duration and restriction of calorie intake but not with reduced carbohydrate content.15
Calorie-controlled restriction diets can be via either a total meal replacement (TMR) or partial meal replacement (PMR) regimen, typically in the form of shakes or bars. The OPTIWIN study involved 273 participants with a BMI of 30−55 kg/m2 and randomised to either the OPTIFAST programme (OP), as a TMR regimen, or a foodbased regimen for 26 weeks. At 26 weeks, average weight loss in the OP group was 12.4±0.6% versus 6.0±0.6% in the food-based group (p<0.001). At 52 weeks, respective percentages compared to baseline were 10.5±0.6% and 5.5±0.6% (p<0.0001), with, importantly, greater fat mass loss in the OP group.16
In a study conducted by Optavia,17 participants followed a PMR regimen comprised of meal replacement products and one low-carb ‘lean and green’ meal and received support through regular coaching calls. When tested against the Metafast diet and a standard food-based diet, the PMR regimen resulted in greater weight loss and adherence, which was proposed to be attributed to the coaching calls.17 These studies highlight the potential utility of controlled, monitored, very low energy (VLE) diets.
Novel Non-pharmacological Weight Loss
Non-pharmacological approaches to weight loss include nutraceuticals and medical devices. Nutraceuticals are food supplements designed to promote weight loss by varying
mechanisms. Some, such as green tea, inhibit, delay, or modify gastrointestinal nutrient absorption. Others act as a metabolic modulator, whey protein being one example, or appetite
regulators, e.g., diacylglycerol, which helps increase fat metabolism. Finally, another category, exemplified by L-carnitine, increase energy metabolism.18
Whey protein stimulates secretion of incretin peptides, particularly glucagon-like peptide (GLP-1), insulin, and gut peptides, resulting in delayed or slowed gastric emptying.19 In the Zeus pilot study20 (N=26; mean BMI: 29.1 kg/m2), 10 g whey protein in the form of a microgel (WPM) was taken as a pre-meal shot, 15 minutes prior to consumption of a test meal. The WPM
significantly augmented GLP-1 response,21 which, according to Neeland, shows that whey protein can act as a GLP-1 agonist and may help reduce glycaemic variability and increase weight loss.22,23 “With this understanding,” Neeland discussed, “things like WPM may be an inexpensive and low risk way to induce GLP-1 agonism in metabolism to improve weight loss and reduce T2D risk.”
Mechanical devices, such as intra-gastric balloons, can be ingested or placed surgically and induce weight loss through increased satiety or alteration of absorption of food contents. While there are several endoscopic weight loss devices available, Neeland advised caution as implantation needs to be carried out under sedation and adverse events though rare, have included bowel perforation, bleeding, obstruction, device migration, and pulmonary aspiration.24
Non-mechanical, expanding, non-caloric ingestible devices essentially produce satiety. One such is Gelesis 100/Plenity® (Gelesis, Boston, Massachusetts, USA), a prescription capsule that contains hydrogel particles that expand in the stomach after ingestion. The particles transit in the gastrointestinal tract, disintegrate, and are excreted. Data show weight loss of
approximately 3−5% compared with standard care.25 The Epitomee® device (not currently approved; Epitomee Medical, Caesarea, Israel) is a biodegradable, encapsulated, shape-shifting device made of absorbent polymers that expands in the stomach to create a super absorbent, pHsensitive gel structure that mimics a large, solid food mass. The device disintegrates into small particles within 30 minutes, minimising the risk for gastric obstruction. In a single-arm pilot study, 52 participants (baseline BMI: 27−40 kg/m2) took the capsule twice daily for 12 weeks and showed weight loss of 3−4% on average.26 Though weight loss was modest with both devices, Neeland pointed out that “the risk for these devices is relatively low so they might be a good choice for a patient who wants to increase their satiety not using pharmacological means.”
To conclude, Neeland highlighted that “while at a population level standpoint BMI is related to adverse cardiometabolic outcomes, for personalised medicine approaches, we need to go beyond BMI to identify those at highest risk who would benefit from therapies in order to decrease any adverse events that might occur.”
Magnetic Resonance Insights to Practical Therapy: Achieving Effective Weight Loss and Remission of Type 2 Diabetes - Roy Taylor
The ‘Personal Fat Threshold’
Hepatic insulin sensitivity is related to the amount of fat in the liver and overnight fasting glucose production, which is found to be higher in people with T2D.27,28 As the liver is responsible for distributing fat throughout the body, Taylor highlighted how, if there is excess fat build-up in the liver because of excess calories, “the speed of that process is increased so excess fat…will silt up in ectopic sites including the pancreas.”27 Excess fat here can lead to metabolic stress in β-cells, causing them to go into “survival mode”, dedifferentiate, and lose their specialist function.27
Historically, T2D development has been associated with obesity; however, in an analysis of data from the UK Prospective Diabetes Study (n=5,102),29 Taylor pointed out how BMI incidence for people with T2D was only slightly skewed from what is considered healthy (<25.0 kg/m2), to a median BMI of 28 kg/m2, with only a relatively minor percentage having a BMI >35 kg/m2.30 In the Nurses’ Health Study, which followed females from early to later life, the relative risk (RR) for developing T2D in people with a BMI <23 kg/m2 compared to those with a BMI ≥35 kg/m2 was very high (RR: 38.8; 95% confidence interval [CI]: 31.9−47.2). However, there was also a notable increase in RR for those with a BMI of 25.0−29.9 kg/m2 (RR: 7.59; 95% CI: 6.27−9.19) or even of 23.0−24.9 kg/m2 (RR: 2.67; 95% CI: 2.13−3.24).31
These findings challenge the idea of a tight relationship between BMI-determined obesity alone being the cause of T2D. Taylor discussed how people should be thinking more about the concept of a PFT and how when a person is carrying more fat than their body has metabolically coped with in the past can lead to crossing a PFT into the zone where T2D develops (Figure 3A, where the dotted line is each person’s PFT). For instance, a male who was underweight aged 21 years who gained weight in middle age but was still not considered overweight at this time could in fact be carrying as much excess fat on his body compared to his 21-year-old self as someone who went from being overweight aged
21 years to being obese in middle age.30 In line with this concept, Taylor presented data showing that a 15 kg weight loss in a person of any weight who develops T2D could restore normal health, and stressed how useful it was to educate patients about their PFT and explain how it is β-cell susceptibility to excess fat that determines T2D risk. This would enable patients that develop T2D, but without obesity, to understand why all people with diabetes need to lose weight to have a chance of remission.
Type 2 Diabetes and Very Low Energy Diets
A number of years ago, Taylor and colleagues postulated that a negative calorie balance should decrease hepatic fat levels, improve pancreatic insulin response, and normalise overnight blood sugar. In the Counterpoint study, 11 people with T2D (not on insulin; <4 years duration; BMI: 33.5±1.2 kg/m2) were given a liquid-based diet (600–800 kcal/day) for 8 weeks. Within the first 7 days, fasting plasma glucose (FPG) normalised (5.9±0.4 mmol/L down from 9.2±0.4 mmol/L) and hepatic triacylglycerol content reduced to 2.9±0.2% from a baseline mean of 12.8±2.4%. By Week 8, FPG remained at normal levels and hepatic triacylglycerol content was down to 2.9±0.2%. Critically, there was a gradual fall in pancreatic fat and a return of normal first-phase insulin response.32 These results, emphasised Taylor, held up the hypothesis of positive effects of substantial weight loss on T2D indices.
Of note in the Counterpoint study, only people who had T2D for <4 years were included. The CounterBALANCE study included 30 people with T2D, ranging in duration from diagnosis from 0.5−23 years, who followed a similar liquid diet (624−700 kcal/day) for 8 weeks then a 2-week stepped introduction to solid food and a 6-month structured, individualised weight maintenance phase.33 In the diet ‘responders’ (FPG <7.0 mmol/L) acute insulin response returned to normal at 10 weeks and remained so at 6 months.33 This was important, noted Taylor, as it showed there was no inevitable progressive β-cell failure.
In the ‘non-responders’ at baseline, acute insulin response was almost zero, with little change over the study period. Taylor highlighted that while responders had an average diabetes duration of 3.8±3.3 years, the non-responders average was 9.8±1.6 years, indicating that time with diabetes may impact how recoverable β-cells are; however, he urged, this doesn’t mean that those with a long duration of T2D will not respond to a VLE diet. In fact, Taylor described two patients from his clinical practice whom after 23 years with T2D achieved normal glycaemia and cessation of all anti-diabetes medications with a VLE diet.
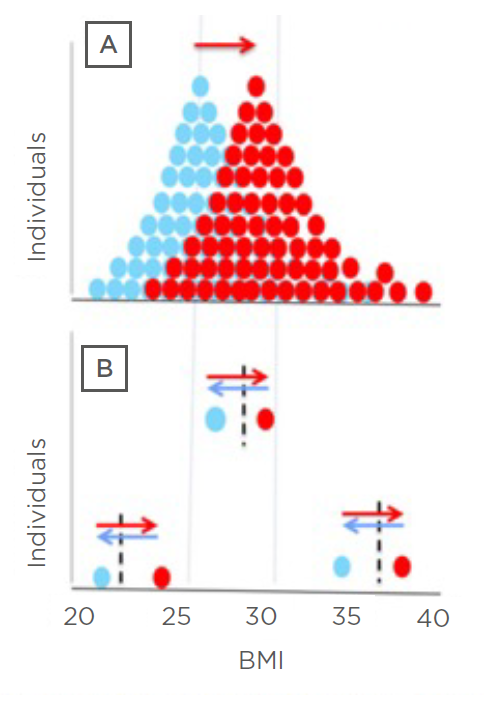
Figure 3: Personal fat threshold.
Representative frequency distribution of BMI for people with Type 2 diabetes before (blue) and after (red) they
gained weight. The frequency distribution indicates a higher prevalence of obesity in this cohort who gained weight.
However, looking at individuals (B), one started out as obese, one overweight, and one normal weight; all lost 15 kg
weight (blue arrows) and returned to normal glucose tolerance once they’d crossed back over their personal fat
threshold, even though their BMI category remained the same.
Adapted from Taylor, Holman.30
With the idea that substantial weight loss could help reverse diabetes, Taylor and colleagues carried out the DiRECT trial to test the feasibility of a VLE diet in routine primary care. Patients with T2D of <6 years duration were randomised to an intervention (n=64) or control (n=26) group. The intervention group stopped all antidiabetic medications on Day 1 of the programme, which consisted of an 825−853 kcal/day liquid formula diet for 12−20 weeks, followed by a 2−6 week food reintroduction phase then ongoing weight-maintenance support. The control group received usual diabetes standard of care.34
At 5 months, while both responders and non-responders lost weight, in responders only, decreases were shown in FPG and HbA1c (to <5.9%), which was maintained at 12 months without medication. In all programme participants, liver fat fell, from approximately 15% to approximately 3%, with pancreas fat falling to a lesser extent. Acute insulin response increased significantly in the responders.34
Another study included participants from DiRECT matched in age, sex, and weight with normoglycaemic controls. This utilised MRI to show that the pancreas in those with T2D was of significantly lower volume than in the normoglycaemic control group prior to the intervention. At 24 months, the pancreas volume of the responders increased to near-normal levels.35 “This gross change in whole pancreas,” stressed Taylor, “really emphasises the nature of remission: it is a return to the normal state, not just well-controlled T2D.”
Also of note in the DiRECT study was how the intervention affected blood pressure. One analysis included a subset of 78 patients in the intervention group (n=143) that were taking antihypertensive medications prior to the start of the study but in whom these were completely (85%) or partially (5%) discontinued on Day 1. By Week 20, SBP decreased approximately 10 mmHg in all sub-groups regardless of whether they had a history of hypertension or discontinued or
remained on their hypertension medications.36
Concerns are often expressed about the safety of a VLE diet; however, Taylor pointed out that of the DiRECT participants who were followed over 24 months, 19 participants (13%) in the control group (n=149) experienced 25 serious adverse
events (SAEs), but there were only 15 SAEs in 11 participants (7%) in the intervention group (n=149). SAEs in the control group included one fatal myocardial infarction, two cerebrovascular disorders, one aortic aneurysm, five weight related cancers, and one toe amputation; in the intervention group there were no fatalities, no amputations, and no cancers.37 “This is nothing to do with the cause of cancer though,” pointed out Taylor, “but with the rate of progression and presentation as insulin is a major factor in promoting tumour growth and inhibiting apoptosis.”
During the Counterpoint study, Taylor discussed how he and his team realised that for many of the participants, success was determined by how on-board and involved their spouse or partner was; hence, it is vital to include a person’s family in a patient’s dietary goals. Another challenge in the earlier studies was that, according to Taylor, while the diet was easier than people expected, the change back to eating solid food was harder. However, Taylor emphasised that the solid food
reintroduction period can serve as a ‘clean slate’ opportunity, whereby specific behavioural and dietary modification education can be provided on what to eat for the long-term to avoid weight regain.
Another factor to be taken into account is how stressful life events can lead to poor weight management and weight gain. In the DiRECT study, participants were offered ‘rescue plans’ whereby if they gained ≥2 kg they would go back onto PMR for 2−4 weeks and if they gained >4 kg they could return to TMR for 4 weeks, followed by 4 weeks food introduction. “In the end,” discussed Taylor, “there was no difference in outcomes in those who required rescue plans and those who didn’t.”37 This was, he suggested, because “weight regain is not a failure or a disaster, it just calls for focused attention when people can re-engage with dietary restriction.” Taylor concluded that at T2D diagnosis, people must be offered a choice of conventional medication therapy or supervised weight loss and potential freedom from diabetes. For this, personal planning, including family members, is essential, and the target should be 15 kg weight loss.
SUMMARY
Overall, both Neeland and Taylor emphasised the need to look beyond BMI and investigate indices of body fat distribution to understand a patient’s risk for developing cardiovascular and metabolic diseases. In those where this is an issue, there are a variety of interventions, with lifestyle modifications being key. Caloric restriction can successfully reduce VIF and reverse T2D, including β-cell dysfunction; however, weight loss is best carried out in a supportive setting with weight maintenance and ‘rescue’ plans in place once the VLE diet part of a programme is finished.
References
1. Arnett DK et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/ American Heart Association task force on clinical practice guidelines. Circulation. 2019;140(11):e596-e646.
2. Neeland IJ et al. Dysfunctional adiposity and the risk of prediabetes and Type 2 diabetes in obese adults. JAMA. 2012;308(11):1150-9.
3. Neeland IJ et al. Cardiovascular and metabolic heterogeneity of obesity: clinical challenges and implications for management. Circulation. 2018;137(13):1391-406.
4. Hales CM et al. Prevalence of obesity among adults and youth: United States, 2015-2016. NCHS Data Brief. 2017;288:1-8.
5. Khan SS et al. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity. JAMA Cardiol. 2018;3(4):280-7.
6. Ofenheimer A et al. Reference values of body composition parameters and visceral adipose tissue (VAT) by DXA in adults aged 18-81 years-results from the LEAD cohort. Eur J Clin Nutr. 2020;74(8):1181-91.
7. Ulbrich EJ et al. Age and gender dependent liver fat content in a healthy normal BMI population as quantified by fat water separating DIXON MR imaging. PLoS One. 2015;10(11):e0141691.
8. American Diabetes Association. Understanding A1c: A1c does it all. 2021. Available at: https://www.diabetes.org/a1c. Last accessed: 11 October 2021.
9. Grundy SM. Small LDL, atherogenic dyslipidemia, and the metabolic syndrome. Circulation. 1997;95(1):1-4.
10. Neeland IJ et al. Body fat distribution and incident cardiovascular disease in obese adults. J Am Coll Cardiol. 2015;65(19):2150-1.
11. Despres JP et al. Management of obesity in cardiovascular practice: JACC focus seminar. J Am Coll Cardiol. 2021;78(5):513-31.
12. Jensen MD et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the obesity society. Circulation. 2014;129(25 Suppl2):S139-40.
13. Gepner Y et al. Effect of distinct lifestyle interventions on mobilization of fat storage pools: CENTRAL magnetic resonance imaging randomized controlled trial. Circulation. 2018;137(11):1143-57.
14. Bhanpuri NH et al. Cardiovascular disease risk factor responses to a Type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: an open label, non-randomized, controlled study. Cardiovasc Diabetol. 2018;17(1):56.
15. Bravata DM et al. Efficacy and safety of low-carbohydrate diets: a systematic review. JAMA. 2003;289(14):1837-50.
16. Ard JD et al. Effectiveness of a total meal replacement program (OPTIFAST Program) on weight loss: results from the OPTIWIN study. Obesity (Silver Spring). 2019;27(1):22-9.
17. Arterburn LM et al. Randomized controlled trial assessing two commercial weight loss programs in adults with overweight or obesity. Obes Sci Pract. 2018;5(1):3-14.
18. Watanabe M et al. Current evidence to propose different food supplements for weight loss: a comprehensive review. Nutrients. 2020;12(9):2873
19. Smith K et al. The clinical application of mealtime whey protein for the treatment of postprandial hyperglycaemia for people with Type 2 diabetes: a long whey to go. FrontNutr. 2020;7:587843.
20. Johansen O et al. Very-low dose pre-meal whey protein microgels reduce postprandial glucose in Type 2 diabetes: a randomised, placebo-controlled crossover study. Abstract 112. European Association for the Study of Diabetes (EASD) Annual meeting, 27 September–1 October, 2021.
21. De Gregorio LH et al. Very-low-dose premeal whey protein microgels reduce postprandial postprandial (pp) glucose in Type 2 diabetes: a randomized, placebo-controlled crossover study. Virtual Session 37-LB. American Diabetes Association 81st Scientific Session, 25–29 June, 2021.
22. Rigamonti AE et al. The appetite suppressant and GLP-1-stimulating effects of whey proteins in obese subjects are associated with increased circulating levels of specific amino acids. Nutrients. 2020;12(3):775.
23. Jakubowicz D et al. High-energy breakfast based on whey protein reduces body weight, postprandial glycemia and HbA(1C) in Type 2 diabetes. J Nutr Biochem. 2017;49:1-7.
24. Bazerbachi F et al. Fluid-filled versus gas-filled intragastric balloons as obesity interventions: a network meta-analysis of randomized trials. Obes Surg. 2018;28(9):2617-25.
25. Greenway FL et al. A randomized, double-blind, placebo-controlled study of Gelesis100: a novel nonsystemic oral hydrogel for weight loss. Obesity (Silver Spring). 2019;27(2):205-16.
26. Shirin H et al. Safety, tolerability and efficacy of a novel selfuse biodegradable device for management of obesity. Obes Sci Pract. 2019;5(4):376-82.
27. Taylor R. Pathogenesis of Type 2 diabetes: tracing the reverse route from cure to cause. Diabetologia. 2008;51(10):1781-9.
28. Singhal P et al. Regulation of endogenous glucose production after a mixed meal in Type 2 diabetes. Am J Physiol Endocrinol Metab. 2002;283(2):E275-83.
29. UK Prospective Diabetes Study (UKPDS). VIII. Study design, progress and performance. Diabetologia. 1991;34(12):877-90.
30. Taylor R, Holman R. Normal weight individuals who develop Type 2 diabetes: the personal fat threshold. Clin Sci (Lond). 2015;1289(7):405-10.
31. Hu FB. et al. Diet, lifestyle, and the risk of Type 2 diabetes mellitus in women. N Engl J Med.2001;345(11):790-7.
32. Lim EL et al. Reversal of Type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia. 2011;54(10):2506-14.
33. Steven S et al. Very low-calorie diet and 6 months of weight stability in Type 2 diabetes: pathophysiological changes in responders and non-responders. Diabetes Care. 2016;39(5):808-15.
34. Taylor R et al. Remission of human Type 2 diabetes requires decrease in liver and pancreas fat content but is
dependent upon capacity for β cell recovery. Cell Metab. 2018;28(4):547-56.e3.
35. Al-Mrabeh A et al. 2-year remission of Type 2 diabetes and pancreas morphology: a post-hoc analysis of the DiRECT open-label, cluster randomised trial. Lancet Diabetes Endocrinol. 2020;8(12):939-48.
36. Leslie WS et al. Antihypertensive medication needs and blood pressure control with weight loss in the diabetes remission clinical trial (DiRECT). Diabetologia. 2021;64(9):1927-38.
37. Lean MEJ et al. Durability of a primary care-led weight-management intervention for remission of Type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol 2019;7(5):344-55



 and Pre-CoMiSS Tool")