Effects of Higher Protein Formula with Improved Fat Blend on Growth and Feeding Tolerance in Preterm Infants

Purpose
To evaluate growth, nutritional status, and feeding tolerance of low birth weight preterm infants fed with either experimental formula (EF) containing 3.4g protein/100kcal, 12.5% of total fat as MCTs, and 40.2% of total palmitic acid esterified in sn-2 position, or control formula (CF) containing 2.9g protein/100 kcal, 30% fat as MCTs, and without enriched sn-2.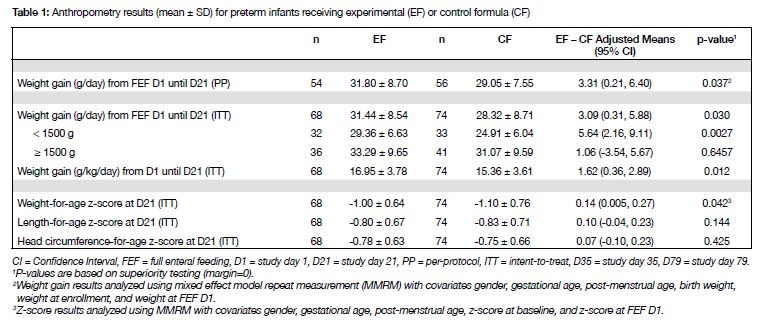
Materials and Methods
Male and female preterm infants with birth weight ≤ 2000g and gestational age ≤33 weeks we recruited from a Neonatal Intensive Care Unit (NICU) at one hospital in Vietnam, and randomized in double-blind manner to receive EF (n = 80) or CF (n = 80) until reaching 3 kg body weight. Differences between groups in weight gain (primary end point) for day 1 (D1) of full enteral feeding (FEF) until D21 were evaluated for non-inferior (margin = –2.5 g/d) and superiority (margin = 0 g/d). Stool consistency was rated on a 5-point scale with higher scores indicating harder stool. Feeding tolerance (including gastrointestinal symptoms and time to reach FEF) and blood / urine biochemistries related to nutritional status were assessed.
Results
Adjusted mean weight gain was 3.1 g/d greater in EF than CF; the lower limit of the 95% CI (0.31 g/d) exceeded both non-inferiority (P=0.0001) and superiority margins (P=0.030). The difference in weight gain was larger among infants <1500g (5.6 g/d; 95% CI = 2.16, 9.11). Fast weight gain in EF (vs. CF) was sustained into the post-discharge phase until D79 (mean difference up to 2.07 g/d). Differences in length-of-rage and head circumference-for-age z-scores at D21 between groups were not significant. There was no group difference in the incidence of gastrointestinal disorders (EF = 21 vs. CF = 18 events), spitting-up / vomiting [EF/CF IRR (95% CI) = 0.57 (0.30, 1.09)] during D1 – D21 period, or time to reach FEF [EF = 16 (15, 17) vs. CF = 15 (13, 17) days]. Infants in the EF group tended to have softer stools [EF = 3.2 ± 0.59 vs. CF = 3.4 ± 0.58; P=0.07]. Serum Blood Urea Nitrogen (BUN) levels were slightly higher in EF vs. CF at D21 [adjusted mean (95% CI); EF = 3.10 (2.89, 3.33); CF = 2.64 (2.46, 2.83), P=0.0015], although all BUN values weer within normal range (1.1 – 7.5 mmol/L). There were no differences between groups in the incidence of abnormal serum creatinine or urinary urea values.Conclusions: EF containing greater protein:energy ratio, enriched sn-2, and reduced MCTs (vs. CF) is safe, nutritionally suitable, well-tolerated, and improves weight gain of preterm infants, especially those with very low birth weight.
If you liked this post you may also like



