Nutrition in Disease Recovery

The topic of nutrition in disease recovery is extremely broad as the impact of nutrition is so great on so many disease processes and outcomes. To take a recent example, the COVID-19 pandemic has shone a light on those in society who are most vulnerable, with many of these groups intersecting with those at the highest nutritional risk in our communities. This chapter will focus on some of the science and physiology underlying the effects of disease on nutritional status and the effects of nutritional status on disease course and recovery.
Infection increases the metabolic demand for energy-yielding substrates (e.g., glucose, amino acids, and fatty acids) to facilitate the production of immune system cells and mediators. These processes also require vitamins and minerals, which act as cofactors in several metabolic reactions. Therefore, an adequate nutritional status contributes to an effective immune response. On the other hand, suboptimal nutritional status might result in blunted responses, as seen in different conditions of macronutrient deficiency.1
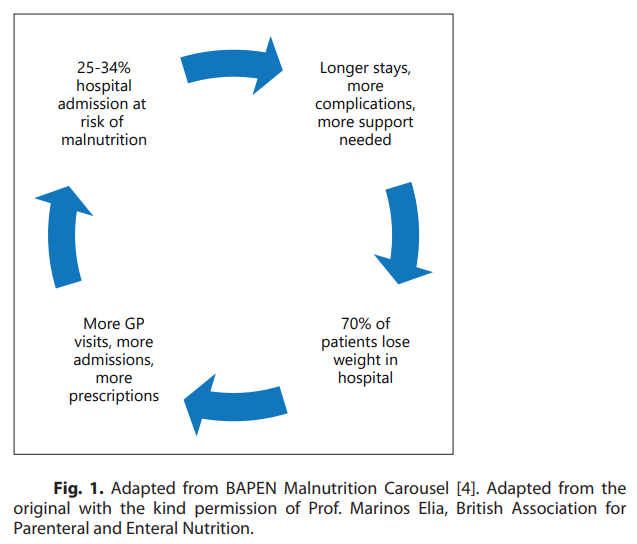
From a public health perspective, the prevalence of malnutrition is evident in the community when patients are admitted to secondary care. Loss of appetite, which often develops during hospitalization, might be either a consequence of an underlying health condition (e.g., pneumonia), medical treatments (e.g., pain medication, chemotherapy), or social factors, such as depression, social isolation, or advanced age. Both acute and chronic illnesses are associated with loss of appetite and poor nutritional intake, frequently accompanied by a proinflammatory state and loss of lean and adipose tissues. Often, patients are discharged from the hospital without adequate nutritional care, which contributes to the cycle of worsened nutritional status, recurrent hospital admissions, and functional decline (Fig. 1).2
Mortality from COVID-19 has been highest among older people and those with comorbidities, who are also often most at risk of malnutrition in society.3 Numerous barriers exist to optimizing nutritional status for those suffering from COVID-19 in the community before ever being admitted to the hospital. These challenges exist more widely across multiple patient groups, related to specific illness-associated nutrition impact symptoms. Accordingly, a focus on nutrition in the rehabilitation process should be an important priority. To promote optimal recovery from illness and build a more resilient population for future health challenges and pandemics, a focus on nutrition increasingly appears to be of paramount importance.4
References
1 Calder PC. Nutrition, immunity and COVID-19. BMJ Nutr Prev Health. 2020 May 20;3(1):74–92.
2 BAPEN. Introduction to malnutrition; 2018. Available from: https://www.bapen.org. uk/malnutrition-undernutrition/introduction-to-malnutrition?start=1
3 Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020 Apr 7;323(13):1239–42.
4 Cawood AL, Walters ER, Smith TR, Sipaul RH, Stratton RJ. A review of nutrition support guidelines for individuals with or recovering from COVID-19 in the community. Nutrients. 2020 Oct 22;12(11):3230.