Nutrition for bone growth in toddlers


Key messages:
• Bone mass evolves across the lifespan but specifically increases during childhood and puberty. Bone fragility (low bone strength) and fracture risk has been associated with high growth rate periods (e.g. toddlerhood and adolescence).
• Adequate intakes of calcium and vitamin D are important for healthy bone growth. Food fortification or supplements may be an effective way to reduce inadequacies.
• There is emerging evidence to suggest a contribution of a healthy microbiome for bone health. Preclinical studies show modulation of bone health by pre- and probiotics but clinical studies are required to confirm these effects in children.
Bone is a “dynamic” and highly specialized connective tissue, the main function being to provide mechanical strength for muscular activity and physical protection to internal organs, as well as to act as a repository for systemic mineral homeostasis (e.g. 99 % of the body’s calcium is in the skeleton). Skeletal growth proceeds through the coordinated action of bone deposition and resorption to allow bones to expand (periosteal apposition of cortical bone) and lengthen (endochondral ossification) into their adult size. This process of bone modeling starts during fetal life and continues after birth until epiphyseal fusion is finished, during early adulthood.1
Periods of rapid growth, i.e. during toddlerhood and adolescence (following onset of puberty), are followed by a rapid bone mineral accretion that peaks shortly after peak height gain.2 During this dynamic period, the skeleton is particularly vulnerable to fracture with a higher frequency reported among children than in young adults, highlighting the increased requirement for adequate nutrient intake to optimize bone strength and peak bone mass. Indeed, understanding factors that affect bone strength in young childhood is important since low bone strength is associated with high fracture risk later in life, bone strength being composed of bone geometry (length & width) and bone mineral content.
In contrast to adults, bone health in children and adolescents is an understudied area, e.g. regarding the effect of lifestyle factors, such as nutrition, to bone density or quality.1 Effects of calcium and vitamin D supplementation on the ageing skeleton have been mainly studied in post-menopausal women with the greatest benefit observed in women with low calcium intakes. In contrast, very few randomized controlled studies (RCTs) in children are available. Most of the RCTs addressing calcium supplementation, whether with pills, fortified foods or dairy, consistently show increased gain in skeletal mass and density in children and adolescents, usually between 1.0 and 5.0 %. Importantly, the bone accrual in the supplemented group was always largest in children who had the lowest intakes of calcium at baseline (e.g. in low or non-dairy drinkers) compared to the control group.3 Similarly, the effects of vitamin D supplementation on childhood and adolescent bone mineral accrual were more pronounced when baseline 25(OH)D was between 18 and 48 nmol/L, which is lower than the 50-nmol/L cutoff used to define vitamin D sufficiency.4 This highlights the importance to reduce micronutrient inadequacy in this population through appropriate fortified foods or supplements.
Nutritional opportunities to address bone growth and strength during childhood beyond Ca and vitamin D include the emerging role of vitamin K2 for bone health, 5 as it is needed to transfer calcium from the blood to the skeleton in complementarity to the role of vitamin D in absorption of intestinal calcium (see Figure 1).
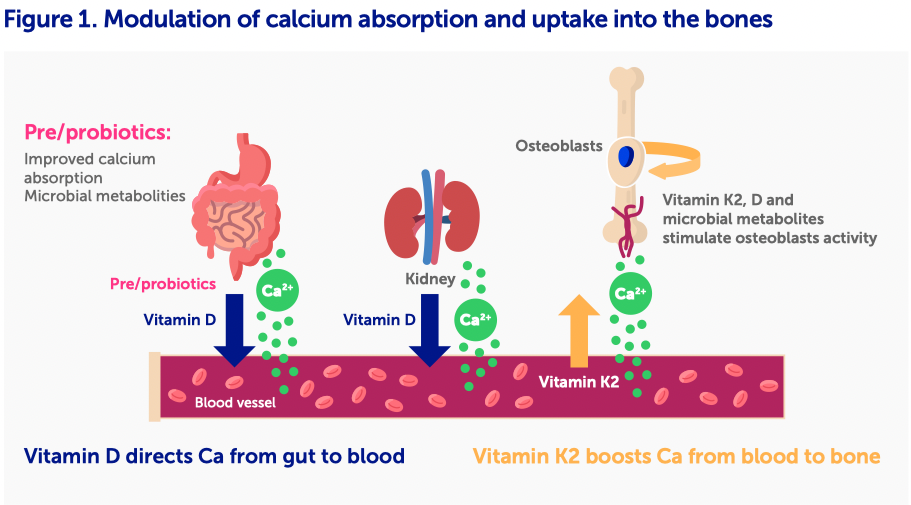
Currently there is a growing interest in the role of pre- and probiotics to modulate bone growth and strength (gut-bone axis) opening a new window of opportunity to support bone health in early life. Several preclinical data suggest that specific (non-digestible) fibers, such as Fructo/Galactooligosaccharides, Inulin, human milk oligosaccharides as well as some probiotics (e.g. L. reuteri, L. rhamnosus...) improve calcium absorption and increase microbial metabolites levels, optimizing bone length, density and strength in growing animals.6 Clinical trials remain, however, to be performed.
In conclusion, childhood represents critical growth periods with rapid bone accretion associated with transient bone fragility but being key to achieve peak bone mass and strength. While there are several emerging dietary factors influencing bone mass and strength, there is a need to strengthen the level of clinical evidence in children.
Acknowledgements:
The authors would like to thank Elizabeth Offord (PhD) and Eline van der Beek (PhD), for critical review of the manuscript.
References
1. Weaver CM, et al., The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int., 2016. 27(4): p. 1281-1386.
2. Zadik Z, Price D, and Diamond G, Pediatric reference curves for multi-site quantitative ultrasound and its modulators. Osteoporos Int, 2003. 14(10): p. 857-62.
3. Specker B and Binkley T, Randomized trial of physical activity and calcium supplementation on bone mineral content in 3- to 5-year-old children. J Bone Miner Res. , 2003. 18(5): p. 885-92.
4. Winzenberg T, et al., Effects of vitamin D supplementation on bone density in healthy children: systematic review and meta-analysis. BMJ, 2011. 342(c7254).
5. van Summeren MJ, et al., The effect of menaquinone-7 (vitamin K2) supplementation on osteocalcin carboxylation in healthy prepubertal children. Br J Nutr. , 2009. 102(8): p. 1171-8.
6. Whisner, C.M. and C.M. Weaver, Prebiotics and Bone. Adv Exp Med Biol, 2017. 1033: p. 201-224.