Introduction of Complementary Foods to Infants
Key insights
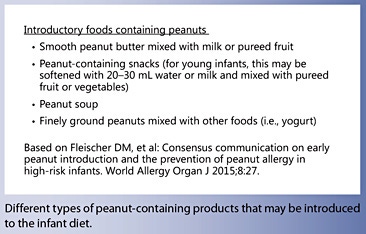
In the past, food allergy prevention strategies focused on the avoidance of allergenic foods in infancy. The current paradigm, however, is shifting from avoidance to controlled exposure. Recent evidence from randomized controlled trials suggests that the early introduction of allergenic foods such as peanuts may reduce the prevalence of food allergies in high-risk infants. In countries where peanut allergy is prevalent, healthcare professionals should recommend the introduction of peanut-containing products into the diets of “high-risk” infants early in life (between 4 and 11 months of age).
Current knowledge
Worldwide, the most common food allergies in children are allergies to cow’s milk, hen’s egg, soy, peanut, tree nuts, wheat, fish, and seafood. Although a large proportion of those with milk or egg allergies will develop tolerance as they age, certain subgroups remain allergic and are at risk of developing other disorders such as respiratory allergic disease. For instance, the presence of both egg allergy and eczema in infants is a predictor of later respiratory allergies. Those with high levels of IgE antibodies to cow’s milk, egg white, wheat, and soy are also more likely to have persistent food allergy.
Practical implications
Current international guidelines state that the introduction of allergenic foods (including egg and peanut) does not need to be postponed beyond 4–6 months of age, but they provide no concrete guidance on whether these foods should be actively introduced within this time frame. The LEAP (Learning Early About Peanut Allergy) trial was the first prospective randomized study regarding early peanut introduction. Results from the LEAP study suggest that early introduction of peanut into the diets of highrisk infants may be beneficial. However, safety and practicality remain key issues when extrapolating the results of this study to the general population. Open questions remain on the optimal timing and doses that should be used, and whether such regimens should be stratified according to the infant’s allergy risk.
Recommended reading
du Toit G, Tsakok T, Lack S, Lack G: Prevention of food allergy. J Allergy Clin Immunol 2016;137:998–1010.

Key Messages
- There is level 1 evidence that early introduction of peanuts (from 4 to 11 months of age) reduces the prevalence of peanut allergy in infants at high risk of allergic disease (infants with severe eczema and/or egg allergy).
- The majority of current international guidelines recommend that complementary foods, including allergenic foods, can be introduced from 4 to 6 months of age irrespective of family history risk.
- As delayed peanut introduction may increase the risk of peanut allergy, interim guidelines state that healthcare providers should recommend introducing peanut-containing products into the diets of “high-risk” infants early on in life (between 4 and 11 months of age) in countries where peanut allergy is prevalent.
Key Words
Eczema · Egg · Food allergy · Infant · Peanut · Prevention · Solid foods
Abstract
While earlier food allergy prevention strategies implemented avoidance of allergenic foods in infancy, the current paradigm is shifting from avoidance to controlled exposure. This review focuses on the outcome of recent randomized controlled trials, which have examined the early introduction of allergenic foods for allergy prevention, and discusses the implementation of results in clinical practice. In infants at high risk of allergic disease, there is now direct evidence that regular early peanut consumption will reduce the prevalence of peanut allergy, compared to avoidance. Many international infant feeding guidelines already recommend complementary foods, including allergenic foods, to be introduced from 4 to 6 months of age irrespective of family history risk. Interim guidelines from 10 International Pediatric Allergy Associations state that healthcare providers should recommend the introduction of peanut-containing products into the diets of infants at high risk of allergic disease in countries where peanut allergy is prevalent. Direct translation of the results obtained from a cohort of high-risk infants to the general population has proved difficult, and issues regarding feasibility, safety, and cost-effectiveness have been raised. Five randomized placebo-controlled trials have assessed the effects of early egg exposure in infancy with varying results. In a recent comprehensive meta-analysis, there was moderate-certainty evidence that early versus late introduction of egg was associated with a reduced egg allergy risk. Although promising, optimal timing, doses, and if the feeding regimen should be stratified according to infant allergy risk remain to be determined. The single study that assessed introduction of multiple foods from 3 months whilst breastfeeding compared with exclusive breastfeeding until 6 months of age showed no reduction in food allergy prevalence. Future research should aim at optimizing infant feeding regimens and support a tolerogenic gastrointestinal microenvironment during the period of food allergen introduction.
Introduction
Over the past few decades, we have experienced a rising prevalence of Immunoglobulin E (IgE)-mediated food allergies in the pediatric setting, particularly in developed countries, although the prevalence also appears to be rising in developing countries [1]. Most reports are based on self-reported food allergy, however, and it has been repeatedly shown that self-reported data will overestimate the prevalence as compared with evaluation by an oral food challenge [2–4]. It is estimated that IgE-mediated food allergy affects approximately 6–8% of children in developed countries [1, 3, 4], thereby posing a significant burden on the afflicted children, their families, and the healthcare system. Globally, the by far most common IgE-mediated food allergies in childhood are allergies to cow’s milk, hen’s egg, soy, peanut, tree nuts, wheat, fish, and seafood [3–5]. Tolerance development is prevalent in milk and egg allergy; and the majority of milk-allergic children [6, 7] and about a half to two-thirds of egg-allergic children [8, 9] will outgrow their food allergy before school age. The rate of peanut allergy resolution is worse; when assessed by oral food challenges both at diagnosis and at follow-up in the Australian HealthNuts cohort study, only 22% of the children outgrew their peanut allergy by 4 years of age [10]. Collectively, a significant proportion of children will remain food allergic and are at risk of developing other comorbidities such as respiratory allergic disease. For instance, infant egg allergy, particularly when coexisting with eczema, has been reported to be a predictor of later respiratory allergies [11], and high levels of IgE antibodies to cow’s milk, egg white, wheat, and soy are predictors of persistent food allergy [12].
Avoidance remains the only available treatment in established food allergy. Oral immune therapy, which includes a stepwise dose increase of the food allergen followed by a maintenance phase, is an emerging treatment option. Oral immune therapy has been demonstrated to induce desensitization, i.e., an increase in the amount of offending food that can be ingested as long as it is consumed regularly [13]. It is still undecided if permanent tolerance will develop, and oral immune therapy is not generally recommended unless within a clinical trials protocol. Adherence to an elimination diet is difficult, and there is still risk of accidental exposure and allergic reactions, including anaphylaxis [14]. Allergic children on elimination diets are also at risk of nutritional deficiencies [15, 16], impaired growth [16–18], and reduced quality of life [19]. Collectively, there is urgent need to develop effective strategies to promote tolerance development and prevent food allergy.
While earlier food allergy prevention strategies implemented food avoidance in early infancy, the current paradigm is shifting from avoidance to controlled exposure
While earlier food allergy prevention strategies implemented food avoidance in early infancy, the current paradigm is shifting from avoidance to controlled exposure. The collective evidence from epidemiological studies reporting an association between delayed introduction of complementary foods and allergy risk, and animal models demonstrating that oral tolerance induction is driven by exposure to antigens and allergens [reviewed in 20 , 21], led to the first randomized controlled trials (RCTs) to examine the role of early, regular exposure to “allergenic” foods for food allergy prevention. This review focuses on the outcome of these recently published RCTs and discusses the implementation of the results in clinical practice.
Risk Factors for Food Allergy
Both genetic and environmental factors will influence the risk of developing food allergy, and multifaceted changes in our modern environment are a likely driver. The hypotheses proposed to explain the epidemic rise in allergic disease include (a) the biodiversity hypothesis, which theorizes that reduced diversity and intensity of microbial exposures will impair normal development of immunoregulatory networks and increase allergy risk [22], (b) the vitamin D hypothesis that builds on epidemiological evidence that vitamin D deficiency is associated with an increased risk of allergic disease, and (c) the dual-barrier hypothesis [23, 24], which is discussed below. There are also data to suggest that food allergens, specific nutrients, lifestyle factors, and microbial exposures may influence the development of allergic disease through epigenetic mechanisms [25].
A commonly used definition of allergy risk is based on a history of allergic disease in a first-degree relative [26] and is frequently used in both epidemiological studies and clinical trials. In some of the recently conducted RCTs, however, only infants with an already established allergic phenotype (eczema and/or manifest egg allergy) were included as they are at an even heightened risk [27, 28] (Table 1). For instance, it has been demonstrated that infant eczema is associated with an increased risk of percutaneous sensitization to environmental food allergens, facilitated by an impaired skin barrier [29]. Normally, a food allergen is introduced to and handled by the immune system in the gut to induce a tolerogenic response to the food protein [20, 30]. Accordingly, the dual-barrier hypothesis theorizes that avoidance of a specific food (such as egg or peanut) can increase the risk of developing food allergy if the infant is still exposed to the food allergen in the environment and is percutaneously sensitized [24].
The “Optimal” Window of Introduction of Complementary Foods for Allergy Prevention
Almost 2 decades ago, the American Academy of Pediatrics Committee on Nutrition launched guidelines suggesting a delayed introduction of dairy products in the first year of life in infants with a family history of allergic disease: egg until 2 years, peanuts, nuts, and fish until 2–3 years of age [31]. This recommendation also became integrated in infant feeding guidelines in many other countries at the time. Following the publication of more recent epidemiological studies across the globe, the guidelines were revised to reflect the lack of solid scientific evidence that delayed introduction of complementary foods beyond 4–6 months of age, or avoidance of “allergenic” foods such as cow’s milk, egg, peanuts, tree nuts, fish, and seafood, reduce allergy risk [32–36]. Still, the “optimal” time for introduction of complementary food for allergy prevention is not known. There are data to suggest that starting complementary foods before 3–4 months of age may increase the risk of allergic disease [37, 38]. At that age, the gut is more permeable and gastrointestinal colonization is not yet well established, which might contribute to the observed risk increase [39, 40]. Consequently, many international infant feeding guidelines for allergy prevention recommend introduction of any solid food after 4 months of age [32–36].
RCTs for Food Allergy Prevention
Peanuts
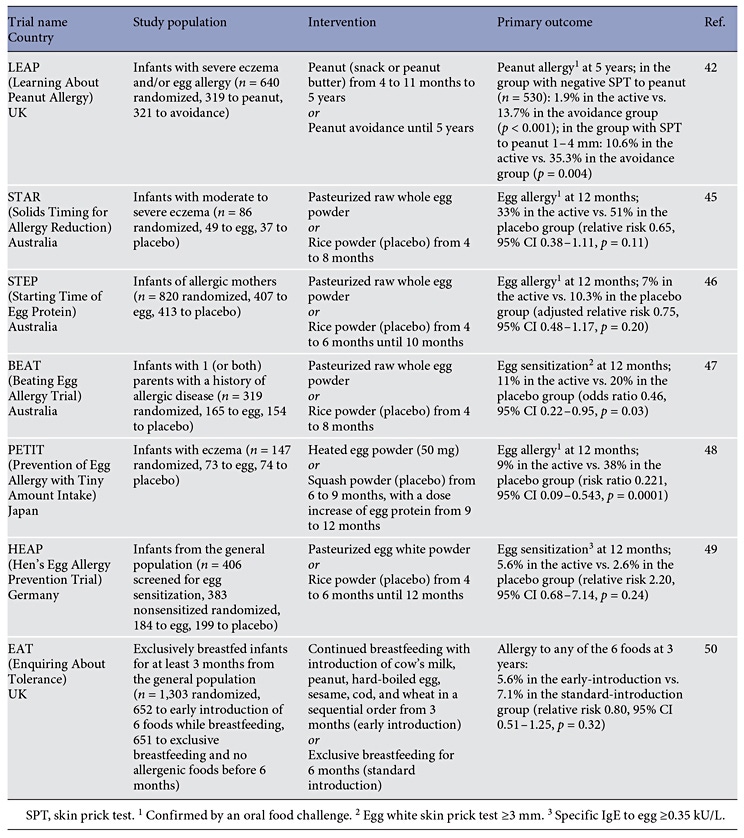
In a cross-sectional study, du Toit et al. [41] found that the prevalence of peanut allergy was 10-fold higher in Jewish children in the UK compared with children in Israel. Interestingly, peanut consumption was initiated earlier and in larger quantities in Israel than in the UK. Based on these findings, the Learning Early About Peanut Allergy (LEAP) study was designed to examine if early, regular, controlled peanut consumption, compared with avoidance, could prevent peanut allergy in high-risk infants with severe eczema, egg allergy, or both [42] (Table 1). As part of the screening, a skin prick test (SPT) to peanut was performed, and infants with a wheal size ≥ 5 mm were excluded. The intervention was initiated between 4 and 11 months and continued until 5 years of age. The study results were pronounced; in the early-introduction group, peanut allergy was reduced with 86% in the group with a negative SPT to peanut at baseline, and with 70% in the group with SPT peanut 1–4 mm at baseline, compared with the avoidance group. Reassuringly, the investigators recently reported that 12-month peanut avoidance in the early-introduction group did not increase the prevalence of peanut allergy at the age of 6 years [43], suggesting that avoidance for a prolonged period will not break tolerance. Still, the long-term consequences of peanut avoidance beyond 12 months are unknown.
Egg
There is also epidemiological evidence to support that delayed introduction of egg to the infant diet increases allergy risk. In the HealthNuts cohort study, delayed introduction of egg at 10–12 months or after 12 months of age was associated with an increased risk of egg allergy compared with egg introduction at 4–6 months of age [44]. To date, 5 RCTs have examined if early versus late introduction of egg can reduce the risk of egg allergy [45– 49] (Table 1). In the Solids Timing for Allergy Reduction (STAR) study, high-risk infants with moderate-to-severe eczema were randomized to intake of pasteurized raw whole egg powder or rice powder (placebo) from 4 to 8 months of age [45]. At 12 months of age, 33% in the active group versus 51% in the placebo group had developed egg allergy (relative risk 0.65, 95% CI 0.38–1.11, p = 0.11). In the Starting Time of Egg Protein (STEP) study, high-risk infants (based on maternal atopy but no allergic manifestation in the infant at baseline) were randomized to intake of pasteurized raw whole egg powder or rice powder (placebo) from 4 to 10 months of age [46]. At 12 months of age, 7% in the active group versus 10.3% in the placebo group had egg allergy (adjusted relative risk 0.75, 95% CI 0.48–1.17, p = 0.20). The Beating Egg Allergy Trial (BEAT) also included high-risk infants (based on allergic disease in any or both parents) [47]. Infants were randomized to pasteurized raw whole egg or rice powder (placebo) from 4 to 8 months of age. The primary outcome was egg sensitization at 12 months of age, and 11% in the active group versus 20% in the placebo group were sensitized (odds ratio 0.46, 95% CI 0.22–0.95, p = 0.03). Twenty-one infants were classified as having probable egg allergy. Of these, 6.2% were in the active group and 10.5% were in the placebo group ( p = 0.20).
In the Prevention of Egg Allergy with Tiny Amount Intake (PETIT) study, high-risk infants with established eczema were randomized to intake of either heated egg powder or squash powder (placebo) from 6 to 12 months of age, with an increased dose of egg protein from 9 months [48]. There was a marked effect of the intervention with egg allergy diagnosed at 12 months in 9% in the active group versus 38% in the placebo group (risk ratio 0.221, 95% CI 0.09–0.543, p = 0.0001). In fact, the striking effect of the intervention in the preplanned interim analyses led the investigators to terminate the trial prematurely. As discussed by the investigators [48] the difference might be biased, leading to a bigger difference between the active and placebo groups than if the study had not been closed.
In contrast to the above-mentioned studies that included high-risk infants, the Hen’s Egg Allergy Prevention (HEAP) study, randomized infants with normal risk (from the general population) to intake of pasteurized egg white powder or rice powder from 4 to 6 months until 12 months of age [49]. Infants were screened for egg sensitization, and all included infants had specific IgE to egg <0.35 kU/L at baseline. As in the BEAT study [47], the primary outcome was egg sensitization at 12 months. 5.6% in the active group were sensitized to egg versus 2.6% in the placebo group (relative risk 2.20, 95% CI 0.68– 7.14, p = 0.24). At that age, 2.1% in the active group had egg allergy versus 0.6% in the placebo group (relative risk 3.30, 95% CI 0.35–31.32, p = 0.35).
Collectively, 4 out of 5 conducted RCTs designed for egg allergy prevention were negative (Table 1), although 3 of these studies [45–47] had nonsignificant results that might suggest a benefit of early egg introduction.
Multiple Foods Approach
Observational studies have also reported an association between low food diversity in early life and both sensitization [50] and allergic manifestations [51]. In the Enquiring About Tolerance (EAT) study [52] (Table 1), 3-month-old breastfed infants from the general population were randomized to continued breastfeeding with introduction of cow’s milk, peanut, hard-boiled egg, sesame, white fish, and wheat in a sequential order from 3 months of age or to continued exclusive breastfeeding for the first 6 months of life [52]. In the intention-totreat analysis, 5.6% of the children in the early-introduction group had developed food allergy at 3 years of age compared to 7.1% in the group that introduced solid foods from the age of 6 months (relative risk 0.80, 95% CI 0.51–1.25, p = 0.32). Of note, only 42% in the earlyintroduction group were able to adhere to the food introduction regimen, demonstrating that it can be difficult to introduce multiple foods as compared to a single food item. In the per protocol analysis, however, the prevalence of “any” food allergy was 2.4% in the earlyintroduction group compared with 7.3% in the standard- introduction group ( p = 0.01). The prevalence of peanut and egg allergy was also reduced in the earlyintroduction group (0 vs. 2.5%, p = 0.003, and 1.4 vs. 5.5%, p = 0.009, respectively). There was no difference between the 2 groups in the prevalence of allergy to milk, sesame, fish, or wheat.
Meta-Analysis of Egg and Peanut Prevention Trials
In a recent comprehensive systematic review and meta-analysis, Ierodiakonou et al. [53] included the trials discussed above that had assessed early versus late egg introduction for egg allergy prevention (5 trials, 1,915 participants) [45–49] (Table 1). They found with moderate certainty evidence that early versus late introduction of egg was associated with a reduced egg allergy risk (risk ratio 0.56, 95% CI 0.36–0.87, p = 0.009). They also identified the LEAP [43] and EAT [52] studies (Table 1) (2 trials, 1,550 participants) to be included in a meta-analysis of early versus late introduction of peanuts and reported that early introduction was associated with a reduced peanut allergy risk (risk ratio 0.29, 95% CI 0.11–0.74, p = 0.009). The authors underscored that the studies were few and that the certainty of the evidence was reduced due to imprecision, indirectness, and heterogeneity in interventions and study populations [53]. An interesting finding, however, was that there was no distinct difference among infants at “normal” versus high risk of allergy in their analyses.
Allergic Reactions and Safety Issues
A shared feature of the studies that included high-risk infants and used pasteurized raw egg powder is that a varying proportion (4.7–31%) of the participants in the early egg intake groups discontinued egg ingestion due to allergic reactions to the egg powder [45–47]. This has raised the question if screening for sensitization would be necessary before introducing egg to the infant diet. Reassuringly, in the STEP trial that included infants with familial predisposition but no eczema, there were no anaphylactic reactions to the egg powder [46]. The authors underscored that assessment of egg sensitization before the introduction of egg and egg-containing products to the infant diet is not necessary in the community setting [46]. In the PETIT trial [48], which included high-risk infants with eczema, a few participants reported mild to moderate allergic manifestations following ingestion of the study powder, but at a similar frequency in the active and placebo groups. No participant discontinued the intervention because of allergic reactions to the egg powder, and it has been argued that this could be a matter of reduced allergenicity of heated versus pasteurized (raw) egg powder [48]. The risk of adverse reactions to peanut was low in the LEAP study; 5% of infants randomized to early peanut intake reacted at the baseline peanut challenge. However, infants at a presumably higher risk (peanut wheal size ≥ 5 mm) were excluded.
Current Recommendations
Current international guidelines already state that introduction of allergenic foods, including egg and peanut, does not need to be postponed beyond 4–6 months of age [32–36]. With a few exceptions, these guidelines do not, however, advocate that allergenic foods should be actively introduced to the infant diet between 4–6 months of age. Based on level 1 evidence from the LEAP study [42], interim guidelines on peanut introduction for allergy prevention in high-risk infants were launched in 2015 ( Table 2 ) [54]. In an opinion paper, Allen and Koplin [55] identified and discussed the challenges in translating the findings from the LEAP study to the general population level. Safety remains one issue, particularly in very highrisk infants, as the LEAP study excluded infants with an SPT to peanut ≥ 5 mm, cost-effectiveness another [55]. Very recently, addendum guidelines for penaut allergy prevention in the United States were launched [56]. In brief, the guideline panel suggests introducing peanuts at home to the majority of infants in the first year of life. Infants with severe eczema, egg allergy, or both should undergo medical assessment including assessment of sensitization to peanut before peanut introduction at 4–6 months of age [56]. If other allergenic foods, such as egg, should also be actively introduced to the infant diet from 4 to 6 months of age remains undetermined. Recent allergy prevention guidelines in Australia now suggest introducing cooked (but not raw) egg from 4 to 6 months of age irrespective of allergic heredity [36]. As underlined by Ierodiakonou et al. [53], the findings from their systematic review on early versus late introduction of complementary foods for allergy prevention cannot be directly translated to new guidelines. Collectively, the optimal timing, doses and form of egg, and if these regimens should be stratified according to the infant’s allergy risk remain to be determined.
Conclusion
The level 1 evidence form the LEAP study [43] has resulted in interim guidelines recommending early introduction of peanut into the diets of “high-risk” infants [54]. Further studies should aim at optimizing infant feeding regimens. Supporting the most favorable “tolerogenic” microenvironment in the gut during the period of food allergen introduction is also likely to involve “optimal” colonization of the gastrointestinal tract, breastfeeding, and other dietary factors with immunomodulatory capacity [39, 40].
Disclosure Statement
The author reports no conflict of interest in relation the topic. The writing of this article was supported by Nestlé Nutrition Institute.
References
- Prescott SL, Pawankar R, Allen KJ, Campbell DE, Sinn J, Fiocchi A, et al: A global survey of changing patterns of food allergy burden in children. World Allergy Organ J 2013; 6: 21.
- Winberg A, West CE, Strinnholm Å, Nordström L, Hedman L, Rönmark E: Assessment of allergy to milk, egg, cod, and wheat in Swedish schoolchildren: a population based cohort study. PLoS One 2015; 10:e0131804.
- Nwaru BI, Hickstein L, Panesar SS, Roberts G, Muraro A, Sheikh A, et al: Prevalence of common food allergies in Europe: a systematic review and meta-analysis. Allergy 2014; 69: 992–1007.
- Rona RJ, Keil T, Summers C, Gislason D, Zuidmeer L, Södergren E, et al: The prevalence of food allergy: a meta-analysis. J Allergy Clin Immunol 2007; 120: 638–646.
- Allen KJ, Koplin JJ: The epidemiology of IgEmediated food allergy and anaphylaxis. Immunol Allergy Clin North Am 2012; 32: 35– 50.
- Host A, Jacobsen HP, Halken S, Holmenlund D: The natural history of cow’s milk protein allergy/intolerance. Eur J Clin Nutr 1995; 49(suppl 1):S13–S18.
- Wood RA, Sicherer SH, Vickery BP, Jones SM, Liu AH, Fleischer DM, et al: The natural history of milk allergy in an observational cohort. J Allergy Clin Immunol 2013; 131: 805–812.
- Sicherer SH, Wood RA, Vickery BP, Jones SM, Liu AH, Fleischer DM, et al: The natural history of egg allergy in an observational cohort. J Allergy Clin Immunol 2014; 133: 492– 499.
- Ohtani K, Sato S, Syukuya A, Asaumi T, Ogura K, Koike Y, et al: Natural history of immediate-type hen’s egg allergy in Japanese children. Allergol Int 2016; 65: 153–157.
- Peters RL, Allen KJ, Dharmage SC, Koplin JJ, Dang T, Tilbrook KP, et al: Natural history of peanut allergy and predictors of resolution in the first 4 years of life: a population-based assessment. J Allergy Clin Immunol 2015; 135: 1257–1266.e1–e2.
- Tariq SM, Matthews SM, Hakim EA, Arshad SH: Egg allergy in infancy predicts respiratory allergic disease by 4 years of age. Pediatr Allergy Immunol 2000; 11: 162–167.
- Savage J, Sicherer S, Wood R: The natural history of food allergy. J Allergy Clin Immunol Pract 2016; 4: 196–203; quiz 4.
- Vazquez-Ortiz M, Turner PJ: Improving the safety of oral immunotherapy for food allergy. Pediatr Allergy Immunol 2016; 27: 117– 125.
- Fleischer DM, Perry TT, Atkins D, Wood RA, Burks AW, Jones SM, et al: Allergic reactions to foods in preschool-aged children in a prospective observational food allergy study. Pediatrics 2012; 130:e25–e32.
- Persson K, Öhlund I, Nordström L, Winberg A, Rönmark E, West CE: Vitamin D deficiency at the Arctic Circle – a study in foodallergic adolescents and controls. Acta Paediatr 2013; 102: 644–649.
- Thomassen RA, Kvammen JA, Eskerud MB, Juliusson PB, Henriksen C, Rugtveit J: Iodine Status and Growth In 0–2-Year-Old Infants With Cow’s Milk Protein Allergy. J Pediatr Gastroenterol Nutr 2016, Epub ahead of print.
- Beck C, Koplin J, Dharmage S, Wake M, Gurrin L, McWilliam V, et al: Persistent food allergy and food allergy coexistent with eczema is associated with reduced growth in the first 4 years of life. J Allergy Clin Immunol Pract 2016; 4: 248–256.e3.
- Winberg A, West CE, Strinnholm Å, Nordström L, Hedman L, Rönmark E: Milk allergy is a minor cause of milk avoidance due to perceived hypersensitivity among schoolchildren in Northern Sweden. Acta Paediatr 2016; 105: 206–214.
- Steensgard A, Bindslev-Jensen C, Nielsen D, Munch M, Dunn Galvin A: Quality of life in childhood, adolescence and adult food allergy: patient and parent perspectives. Clin Exp Allergy 2016, Epub ahead of print.
- Bryce PJ: Balancing tolerance or allergy to food proteins. Trends Immunol 2016; 37: 659–667.
- Nowak-Wegrzyn A, Szajewska H, Lack G: Food allergy and the gut. Nat Rev Gastroenterol Hepatol 2017;14:241–257.
- Haahtela T, Holgate S, Pawankar R, Akdis CA, Benjaponpitak S, Caraballo L, et al: The biodiversity hypothesis and allergic disease: world allergy organization position statement. World Allergy Organ J 2013; 6: 3.
- du Toit G, Tsakok T, Lack S, Lack G: Prevention of food allergy. J Allergy Clin Immunol 2016; 137: 998–1010.
- Lack G: Update on risk factors for food allergy. J Allergy Clin Immunol 2012; 129: 1187–1197.
- Harb H, Renz H: Update on epigenetics in allergic disease. J Allergy Clin Immunol 2015; 135: 15–24.
- Muraro A, Dreborg S, Halken S, Host A, Niggemann B, Aalberse R, et al: Dietary prevention of allergic diseases in infants and small children. Part II. Evaluation of methods in allergy prevention studies and sensitization markers. Definitions and diagnostic criteria of allergic diseases. Pediatr Allergy Immunol 2004; 15: 196–205.
- Nguyen TA, Leonard SA, Eichenfield LF: An update on pediatric atopic dermatitis and food allergies. J Pediatr 2015; 167: 752–756.
- Greenhawt MJ, Fleischer DM, Atkins D, Chan ES: the complexities of early peanut introduction for the practicing allergist. J Allergy Clin Immunol Pract 2016; 4: 221–225.
- Brough HA, Liu AH, Sicherer S, Makinson K, Douiri A, Brown SJ, et al: Atopic dermatitis increases the effect of exposure to peanut antigen in dust on peanut sensitization and likely peanut allergy. J Allergy Clin Immunol 2015; 135: 164–170.
- Smith KM, Eaton AD, Finlayson LM, Garside P: Oral tolerance. Am J Respir Crit Care Med 2000; 162:S175–S178.
- American Academy of Pediatrics: Committee on Nutrition: Hypoallergenic infant formulas. Pediatrics 2000; 106: 346–349.
- Fewtrell M, Bronsky J, Campoy C, et al: Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J Pediatr Gastroenterol Nutr 2017; 64: 119– 132.
- Muraro A, Halken S, Arshad SH, Beyer K, Dubois AE, Du Toit G, et al: EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy. Allergy 2014; 69: 590–601.
- Greer FR, Sicherer SH, Burks AW: Effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas. Pediatrics 2008; 121: 183–191.
- Chan ES, Cummings C; Canadian Paediatric Society, Community Paediatrics Committee and Allergy Section: Dietary exposures and allergy prevention in high-risk infants: a joint statement with the Canadian Society of Allergy and Clinical Immunology. Paediatr Child Health 2013; 18: 545–554.
- http://www.allergy.org.au/health-professionals/ papers/ascia-guidelines-for-infantfeeding- and-allergy-prevention (accessed January 3, 2017).
- Forsyth JS, Ogston SA, Clark A, Florey CD, Howie PW: Relation between early introduction of solid food to infants and their weight and illnesses during the first two years of life. BMJ 1993; 306: 1572–1576.
- Zutavern A, Brockow I, Schaaf B, Bolte G, von Berg A, Diez U, et al: Timing of solid food introduction in relation to atopic dermatitis and atopic sensitization: results from a prospective birth cohort study. Pediatrics 2006; 117: 401–411.
- West CE, D’Vaz N, Prescott SL: Dietary immunomodulatory factors in the development of immune tolerance. Curr Allergy Asthma Rep 2011; 11: 325–333.
- Simonyte Sjödin K, Vidman L, Rydén P, West CE: Emerging evidence of the role of gut microbiota in the development of allergic diseases. Curr Opin Allergy Clin Immunol 2016; 16: 390–395.
- du Toit G, Katz Y, Sasieni P, Mesher D, Maleki SJ, Fisher HR, et al: Early consumption of peanuts in infancy is associated with a low prevalence of peanut allergy. J Allergy Clin Immunol 2008; 122: 984–991.
- du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, et al: Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015; 372: 803–813.
- du Toit G, Sayre PH, Roberts G, Sever ML, Lawson K, Bahnson HT, et al: Effect of Avoidance on Peanut Allergy after Early Peanut Consumption. N Engl J Med 2016; 374: 1435–1443.
- Koplin JJ, Osborne NJ, Wake M, Martin PE, Gurrin LC, Robinson MN, et al: Can early introduction of egg prevent egg allergy in infants? A population-based study. J Allergy Clin Immunol 2010; 126: 807–813.
- Palmer DJ, Metcalfe J, Makrides M, Gold MS, Quinn P, West CE, et al: Early regular egg exposure in infants with eczema: a randomized controlled trial. J Allergy Clin Immunol 2013; 132: 387–392.e1.
- Palmer DJ, Sullivan TR, Gold MS, Prescott SL, Makrides M: Randomized controlled trial of early regular egg intake to prevent egg allergy. J Allergy Clin Immunol 2017;139: 1600–1607.e2.
- Wei-Liang Tan J, Valerio C, Barnes EH, Turner PJ, Van Asperen PA, Kakakios AM, et al: A randomized trial of egg introduction from 4 months of age in infants at risk for egg allergy. J Allergy Clin Immunol 2017;139: 1621–1628.e8.
- Natsume O, Kabashima S, Nakazato J, Yamamoto- Hanada K, Narita M, Kondo M, et al: Two-step egg introduction for prevention of egg allergy in high-risk infants with eczema (PETIT): a randomised, double-blind, placebo-controlled trial. Lancet 2017;389: 276–286.
- Bellach J, Schwarz V, Ahrens B, Trendelenburg V, Aksunger O, Kalb B, et al: Randomized placebo-controlled trial of hen’s egg consumption for primary prevention in infants. J Allergy Clin Immunol 2017;139: 1591–1599.e2.
- Nwaru BI, Takkinen HM, Niemela O, Kaila M, Erkkola M, Ahonen S, et al: Introduction of complementary foods in infancy and atopic sensitization at the age of 5 years: timing and food diversity in a Finnish birth cohort. Allergy 2013; 68: 507–516.
- Nwaru BI, Takkinen HM, Kaila M, Erkkola M, Ahonen S, Pekkanen J, et al: Food diversity in infancy and the risk of childhood asthma and allergies. J Allergy Clin Immunol 2014; 133: 1084–1091.
- Perkin MR, Logan K, Tseng A, Raji B, Ayis S, Peacock J, et al: Randomized trial of introduction of allergenic foods in breast-fed infants. N Engl J Med 2016; 374: 1733–1743.
- Ierodiakonou D, Garcia-Larsen V, Logan A, Groome A, Cunha S, Chivinge J, et al: Timing of allergenic food introduction to the infant diet and risk of allergic or autoimmune disease: a systematic review and meta-analysis. JAMA 2016; 316: 1181–1192.
- Fleischer DM, Sicherer S, Greenhawt M, Campbell D, Chan E, Muraro A, et al: Consensus communication on early peanut introduction and the prevention of peanut allergy in high-risk infants. J Allergy Clin Immunol 2015; 136: 258–261.
- Allen KJ, Koplin JJ: Does LEAP change the screening paradigm for food allergy in infants with eczema? Clin Exp Allergy 2016; 46: 42–47.
- Togias A, Cooper SF, Acebal ML, et al: Addendum guidelines for the prevention of peanut allergy in the United States: report of the National Institute of Allergy and Infectious Diseases – sponsored expert panel. J Allergy Clin Immunol 2017;139:29–44.