FITS and KNHS Overview: Methodological Challenges in Dietary Intake Data Collection among Infants, Toddlers, and Children in Selected Countries

Abstract
The FITS (Feeding Infants and Toddlers Study) and KNHS (Kids Nutrition and Health Study) are large-scale cross-sectional surveys designed to explore eating patterns, nutrient intakes, and food sources of nutrients among infants and children. FITS and KNHS use data from national surveys when available, but when data are not available for age groups of interest, we collect data using similar methods. So far, we have applied a common analysis approach in Australia, China, Mexico, the Philippines, Russia, and the United States. Although dietary data collection methods shared similarities, other aspects of the survey methodology differed considerably. Food composition tables varied, limiting accurate intake estimates to a short list of nutrients in some countries. Age groups and food grouping systems were not consistent, and the level of detail varied. Not all surveys recorded details about the meals or times when foods were consumed. Nonetheless, the FITS and KNHS have standardized age categories and food groupings, so comparisons can be made, and we have imputed missing values to complete data sets for nutrients of interest. We have also supported primary data collection to fill gaps. This manuscript provides an overview of the individual studies and country data that comprise the current FITS and KNHS.
Introduction to FITS and KNHS
The FITS (Feeding Infants and Toddlers Study) began in 2002 as a large-scale national telephone survey to study the eating patterns and nutrient intakes of infants and young children in the USA [1]. It was followed in 2008 by a second FITS, which surveyed 3,273 infants, toddlers, and preschool children from birth to the age of 4 years [2]. Both studies helped to fill a gap in knowledge of young child eating behaviors and confirmed Nestlé’s commitment to understanding dietary patterns among infants and children during these nutritionally important life stages.
Building on the FITS model, Nestlé expanded this research program to include older children and launched the KNHS (Kids Nutrition and Health Study) in 2014. Together, FITS and KNHS investigate nutrient intakes, food groups consumed, food sources of nutrients, meal patterns, feeding practices, household demographic factors, and key behaviors related to energy intake and expenditure in infants and children in different countries around the world. To date, we have conducted studies in Australia, China, Mexico, the Philippines, Russia, and the USA and plan to continue to expand this research initiative.
Scientific Approach
The FITS and KNHS research program uses a 3-tiered scientific approach (Fig. 1). The first step begins with an understanding of the currently available data in a country or region, informed by a literature review or from other data sources such as data briefs or summary data tables from national surveys. This “nutritional landscaping” helps to identify potential data sources for further analysis and clarify research gaps, but it may also be used to explore topics relevant to the FITS and KNHS research program. An example is the systematic review performed on parenting styles, feeding styles, and feeding practices of children [3]. The second approach we use is to conduct further analysis of national nutrition survey data when available. National nutrition and health surveys are a rich source of information on dietary intakes, and many countries have comprehensive survey data that can be used to further investigate eating patterns and dietary intakes of infants and children. The third approach is to conduct studies in countries where national nutrition surveys do not include age groups of our interest.
National survey data have been used for KHNS in the USA, Australia, and China, and for FITS and KNHS in Mexico, Russia, and the Philippines. In the USA, data from NHANES (the National Health and Nutrition Examination Survey) were used to evaluate meal [4] and snacking patterns [5], energy and protein distribution over the day [6], sedentary behaviors, and functional strength [7]. In Australia, we used data from 3 national surveys to evaluate the energy contribution and foods consumed as snacks over time (1995, 2007, and 2011–2012) [8], and we used the most recent National Nutrition and Physical Activity Survey (NNPAS) to identify meal-specific opportunities to improve dietary intakes for adolescents [9]. The China Health and Nutrition Survey (CHNS) was used to explore health issues related to diet and cardio- metabolic risk factors [10] and the double burden of under- and overnutrition and nutrient adequacy of Chinese children [11]. A longitudinal study investigated the impact of snacking on body mass index in children 2–13 years of age [12]. We also identified micronutrient gaps in the diet [13] and investigated urban-rural disparities in energy intake of Chinese school children 4–17 years of age [14].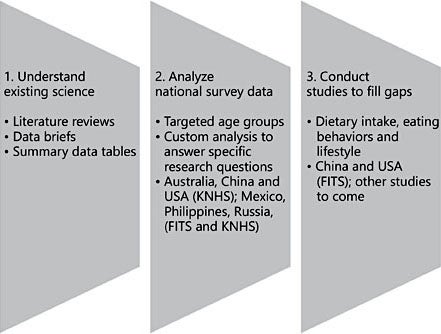
Fig. 1. Three-tiered scientific approach for FITS and KNHS.
National survey data in Mexico (Encuesta Nacional de Salud y Nutrición; ENSANUT 2012) include both infant and child participants, allowing research in both FITS and KNHS age groups. In infants and toddlers, we examined early feeding patterns, documenting low breastfeeding rates and early introduction of complementary foods and cow’s milk [15]. We also found that along with traditional dishes, like soups, beans, tortilla dishes, and eggs, many Mexican infants and young children also consumed sweets (like cookies and sweetened breads) and sweetened beverages [16]. These findings, along with other publications using ENSANUT data, were instrumental in supporting the development of Mexican complementary feeding guidelines [17]. Using data from ENSANUT, we also studied dietary patterns in older children, associating in- creased snacking and eating occasions with higher energy intakes in older (6- to 13-year-old) but not younger (2- to 5-year-old) children [18]. We found that out-of-home food consumption was low overall with only 11% of daily energy coming from out-of-home sources among younger children and 18% for older children [19]. We also evaluated breakfast dietary patterns, characterizing 6 different patterns of consumption, and documented the extent of breakfast skip- ping in Mexican children (14 and 18% among children 4–8 and 9–13 years old, respectively) [20].
The FITS and KNHS project sponsored the Russian Institute of Nutrition to analyze data from the 2013 Russian National Nutrition Survey to evaluate dietary intakes and nutrient adequacy in infants and children [21, 22]. Work is also underway to analyze data from the Philippines 8th National Nutrition Survey 2013–14 (Food and Nutrition Research Institute, the Philippines).
Where national nutrition surveys do not include age groups of our interest, we have conducted our own studies. The Maternal Infant Nutrition Growth (MING) study in China included 1,409 children 6–36 months of age recruited from maternal and childcare centers in 8 major cities. We found low dietary diversity in the diets of infants and young children, with only 5 foods (i.e., fortified milk, rice, noodles, pork, and eggs) contributing 52–69% of daily energy [23]. Fruit and vegetable consumption was low, especially among infants [24]. The diets of Chinese infants and toddlers <24 months of age were generally low in fat, vitamin B6, and folate, and the diets of infants <12 months of age were also low in iron [25].
A third US FITS was completed in 2016. This study included 3,235 infants and young children up to 48 months of age, and the sample was weighted to be nationally representative [26]. The survey instruments were similar to those used in 2008 for purposes of comparability, but some aspects of the methodology were changed. For example, although telephone 24-h recalls were completed on all participants, we recruited subjects both via telephone and online [26], whereas only telephone recruitment was used in 2008 [2]. We also updated the food grouping scheme to be more aligned with the NHANES What We Eat in America food groups. First results from the study show that nutrient intakes are largely adequate, but low iron intakes in 6- to 11-month-old infants are of concern. High sodium intakes and low intakes of potassium, fiber, and vitamin D are issues for toddlers and preschool children [27]. Other publications to share findings from FITS 2016 are under development.
Cross-Country Comparisons
Additional perspective on dietary intakes can be gained by comparing results across countries. For example, there are global recommendations for exclusive breastfeeding for the first 6 months of life, but the foods used for complementary feeding differ by culture and region. When comparing complementary feeding practices, we found higher infant consumption of fruits and vegetables in the USA compared to Mexico or China, largely driven by consumption of baby foods [28]. Rice was widely consumed by infants in China, whereas the major grain source consumed by infants in the USA was infant cereal. Desserts and sweets, including sweetened beverages, were introduced early in Mexico and the USA, but they were virtually absent from the diets of young children in China [28]. Food consumption patterns are established early in life and influence the development of food preferences. We have seen evidence of that with sweets, where we found low consumption of total and added sugars in 4- to 13-year-old children in China representing 8% of total energy intake (TEI), whereas total and added sugars contributed 20 and 26% of TEI in Mexico and the USA, respectively [29], mirroring exposure to sweets in the diets of infants and young children. Snacking patterns also differ by country [30]. In the USA and Australia, snacking is part of the usual dietary pattern of 4- to 13-year-old children (>95% consume snacks on a given day). Snacks account for one-third and one-quarter of TEI in Australia and the USA, respectively. A different pattern is observed in Mexico (76% consume snacks, providing 15% TEI) and in China (65% consume snacks; providing 10% TEI). One important insight from this research was the prevalent consumption of fruits, milk, and water during snacks, which helps to dispel the myth that all snacking is bad. Of course, there is room for improvement, but the snacking occasion can also be a time to promote more consumption of fruits, dairy, and whole-grain-containing foods.
Methodological Similarities and Challenges
In each FITS and KNHS country, dietary intake was assessed using trained in- terviewers and multiple-pass 24-h recalls on one or more days (Table 1). The FITS and KNHS used data from national nutrition and health surveys when available. This was the case for Australia (KNHS), China (KNHS), Mexico (FITS and KNHS), the Philippines (FITS and KNHS), Russia (FITS and KNHS), and the USA (KNHS). In China and the USA, the national surveys did not include infants or toddlers, so we collected data using similar methods (MING in China; FITS in the USA).
A common analysis approach has been applied across data from these countries. Our standard analysis evaluates population nutrient intakes by looking at means and distributions of intakes, and compares them with established dietary reference intakes, including the estimated average requirements, adequate in- take, and tolerable upper intake level. In addition to nutrients, we evaluate meal patterns, including the percent consuming different meals and snacks, the per- cent skipping different meals and snacks, and timing of consumption. Food groups are applied to all foods and beverages reported, and these are then used to look at eating patterns, including the complementary feeding transition, and to understand the top sources of energy and nutrients in the diet.
Although many countries with comprehensive national nutrition surveys use dietary recalls for individual-level intake estimations, other aspects of the survey methodology differ considerably. One of the most apparent is differences in the dietary data collection itself. Two 24-h recalls on nonconsecutive days were used in Australia, the Philippines, and the USA. In China (CHNS), 3 consecutive 24-h recalls were collected. With multiple days of intake, it was possible to estimate usual nutrient intakes, and we have done this in our research. Without multiple days of intake and the application of a usual nutrient intake algorithm, one could overestimate the proportion of the population at the tails of the intake distribution. In the case of China MING, we, therefore, presented only population means and medians for nutrient intakes [25]. The national survey in Russia is very different from the other countries we have studied because they collected 2 days of dietary intake, but 1 day is in the spring and the other in autumn [22]. We have treated these as independent days; otherwise, we would not have been able to properly classify many of the younger children by age [21].
As much as possible, the FITS and KNHS have standardized reporting of age categories and food groupings so comparisons could be made. Typical age categories for FITS and KNHS reporting are 0–5.9, 6–11.9, 12–23.9, and 24–47.9 months, and 4–8 and 9–13 years of age. In some countries, we also study adolescents, depending on the research questions. These age classifications allow us to see details of the transition from an all-milk diet in infancy to foods of the family table, and to a more autonomous food choice in older children.
Aligning food groups is more challenging as the specificity needed for some food groups differs depending on the country. For example, cow’s milk is available in the USA as skimmed, 1% fat, 2% fat, and full-fat milk, and it is also avail- able unflavored and flavored. In contrast, reduced fat milk is virtually nonexistent in China, so this level of detail in the food grouping scheme is not needed there. However, since we were interested in comparing eating patterns across countries, it was necessary to align on food grouping schemes. For example, we recoded all of the foods reported in China’s CHNS to the US Department of Agriculture (USDA) food grouping system used for NHANES [12]. For the re- search on cross-country snacking patterns, higher levels of the USDA food grouping system were aligned to compare food groups consumed during snacks in Australia, China, Mexico, and the USA [30].
We found differences in the lists of nutrients available in food composition tables from different countries. For example, Australia and the USA have very comprehensive food composition tables, whereas the Mexican food composition table was built using a combination of Mexican and other central-American databases (67% of foods), and the food composition tables from the USDA Nutrient Database for Dietary Studies and the USDA National Nutrient Database for Standard Reference, Release 26 (33% of foods) [20]. We imputed missing values to complete data sets for nutrients of interest (e.g., added sugars for Mexico [20] and China [30]). The Philippines are currently in the process of imputing nutrient values, including fiber, sodium, and total sugar, to complete their food composition tables.
Infant feeding practices, eating behaviors, sedentary and physical activities, and sleep are important behavioral and lifestyle attributes that may impact dietary intake and energy expenditure. The extent to which these topics can be explored in FITS and KNHS depends on the data collected in each survey. Child physical activity, time spent in sedentary activities including screen time, and amount and quality of sleep are being evaluated in US FITS 2016 and will be measured in upcoming studies.
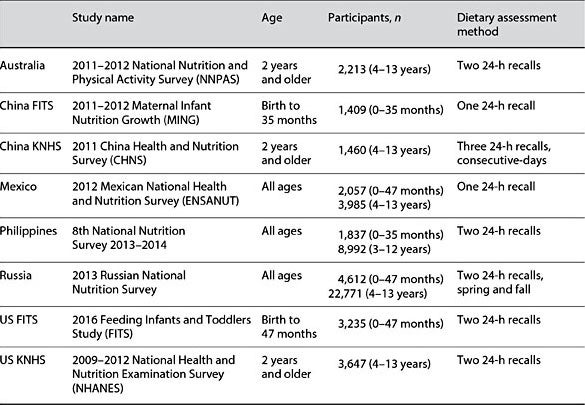
Table 1. FITS and KNHS study countries, sources of data, participant characteristics, and dietary assessment method used
Summary and Recommendations
The FITS and KNHS form a global research initiative to study dietary intakes and related eating behaviors in infants, toddlers, and children. We have evaluated national survey data where they exist, and when not available, we have conducted our own studies to fill the gap in knowledge. Countries currently involved in the project include Australia, China, Mexico, the Philippines, Russia, and the USA. The FITS and KNHS are ongoing and will be expanded to include other countries in the future. Although all of these countries collected dietary intake data using one or more 24-h recalls, we found important methodological differences among the surveys. Food composition tables also varied by country, limiting accurate intake estimates to a short list of nutrients in some places. Different countries used different age classifications and different food grouping schemes, making comparisons across countries more difficult. Not all surveys recorded details about the meals or times when foods were consumed.
To address these issues, we have implemented a common analysis approach, supported work to impute nutrient values to complete food composition databases, and harmonized food grouping systems so comparisons could be made across countries. We further recommend that national surveys include all ages, including infants and young children, to be sure we have data from these vulnerable age groups. The quality of 24-h recall data is very important, with better results achieved through the use of the automated multiple-pass methodology, first developed by the USDA and now in use in Australia, Mexico, and our own US FITS. Multiple days of dietary recalls or records are needed to properly apply the statistical algorithms to estimate usual nutrient intakes of a population. This approach is recommended if we want to more accurately estimate the distributions of intakes in our study samples. Dietary intake data are self-reported and not without limitations, but quality can be enhanced with rigorous methodology, making it a valuable resource for dietary guidance and for informing public health policy.
References
-
1 Devaney B, Kalb L, Briefel R, et al: Feeding Infants and Toddlers Study: overview of the study design. J Am Diet Assoc 2004;104:S8– S13.
-
2 Briefel RR, Kalb LM, Condon E, et al: The Feeding Infants and Toddlers Study 2008: study design and methods. J Am Diet Assoc 2010;110:S16–S26.
-
3 Shloim N, Edelson LR, Martin N, Hetherington MM: Parenting styles, feeding styles, feeding practices, and weight status in 4- to 12-year-old children: a systematic review of the literature. Front Psychol 2015;6:1849.
-
4 Mathias KC, Jacquier E, Eldridge AL: Missing lunch is associated with lower intakes of micronutrients from foods and beverages among children and adolescents in the Unit- ed States. J Acad Nutr Diet 2016;116:667–676.
-
5 Wang D, van der Horst K, Jacquier E, El- dridge AL: Snacking among US children: patterns differ by time of day. J Nutr Educ Behav 2016;48:369–375.
-
6 Mathias KC, Almoosawi S, Karagounis LG: Protein and energy intakes are skewed to- ward the evening among children and adolescents in the United States: NHANES 2013– 2014. J Nutr 2017;147:1160–1166.
-
7 Edelson LR, Mathias KC, Fulgoni VL III, Karagounis LG: Screen-based sedentary behavior and associations with functional strength in 6- to 15-year-old children in the United States. BMC Public Health 2016;16: 116.
-
8 Fayet-Moore F, Peters V, McConnell A, et al: Weekday snacking prevalence, frequency, and energy contribution have increased while foods consumed during snacking have shifted among Australian children and adolescents: 1995, 2007 and 2011–12 National Nutrition Surveys. Nutr J 2017;16:65.
-
9 Fayet-Moore F, McConnell A, Kim J, Mathias KC: Identifying eating occasion-based opportunities to improve the overall diets of Australian adolescents. Nutrients 2017;9:608.
-
10 Piernas C, Wang D, Du S, et al: Obesity, non-communicable disease (NCD) risk factors and dietary factors among Chinese school-aged children. Asia Pac J Clin Nutr 2016;25: 826–840.
-
11 Piernas C, Wang D, Du S, et al: The double burden of under- and overnutrition and nutrient adequacy among Chinese preschool and school-aged children in 2009–2011. Eur J Clin Nutr 2015;69:1323–1329.
-
12 Smith Taillie L, Wang D, Popkin BM: Snacking is longitudinally associated with declines in body mass index z scores for overweight children, but increases for underweight children. J Nutr 2016;146:1268–1275.
-
13 Wang H, Wang D, Ouyang Y, et al: Do Chinese children get enough micronutrients? Nutrients 2017;9:397.
-
14 Zhang J, Wang D, Eldridge AL, et al: Urban- rural disparities in energy intake and contribution of fat and animal source foods in Chinese children aged 4–17 years. Nutrients 2017;9:526.
-
15 Deming DM, Afeiche MC, Reidy KC, et al: Early feeding patterns among Mexican babies: findings from the 2012 National Health and Nutrition Survey and implications for health and obesity prevention. BMC Nutr 2015;1:40.
-
16 Denney L, Afeiche MC, Eldridge AL, Villal- pando-Carrión S: Food sources of energy and nutrients in infants, toddlers, and young children from the Mexican National Health and Nutrition Survey 2012. Nutrients 2017;9:494.
-
17 Romero-Velarde E, Villalpando S, Pérez- Lizaur A, et al: Consenso para las prácticas de alimentación complementaria en lactantes sanos. Guidelines for complementary feeding in healthy infants. Bol Med Hosp Infant Mex 2016;73:338–356.
-
18 Smith Taillie L, Afeiche MC, Eldridge AL, Popkin BM: Increased snacking and eating occasions are associated with higher energy intake among Mexican children aged 2–13 years. J Nutr 2015;145:2570–2577.
-
19 Smith Taillie L, Afeiche MC, Eldridge AL, Popkin BM: The contribution of at-home and away-from-home food to dietary intake among 2- to 13-year-old Mexican children. Public Health Nutr 2017;20:2559–2568.
-
20 Afeiche MC, Smith Taillie L, Hopkins S, et al: Breakfast dietary patterns among Mexican children are related to total-day diet quality. J Nutr 2017;147:404–412.
-
21 Martinchik AN, Keshabyants EE, Baturin AK, et al: The practice of feeding infants of the first year of life in Russia (analysis of data of the Russian Federal State Statistics Service [Rosstat, 2013]) (in Russian). Vopr Det Dietol (Pediatric Nutr) 2017;15:5–11.
-
22 Martinchik AN, Baturin АK, Keshabyants EE, et al: Dietary intake analysis of Russian children 3–19 years old (in Russian). Voprosy Pitaniia (Problems Nutr) 2017;86:50–60.
-
23 Wang H, Denney L, Zheng Y, et al: Food sources of energy and nutrients in the diets of infants and toddlers in urban areas of China, based on one 24-hour dietary recall. BMC Nutr 2015;1:19.
-
24 Yu P, Denney L, Zheng Y, et al: Food groups consumed by infants and toddlers in urban areas of China. Food Nutr Res 2016;60:30289.
-
25 Chen C, Denney L, Zheng Y, et al: Nutrient intakes of infants and toddlers from maternal and child care centres in urban areas of Chi- na, based on one 24-h dietary recall. BMC Nutr 2015;1:23.
-
26 Anater AS, Catellier DJ, Levine BA, et al: The Feeding Infants and Toddlers Study (FITS) 2016: study design and methods. J Nutr 2018; 148:1516S–1524S.
-
27 Bailey RL, Catellier D, Jun S, et al: Total usual nutrient intakes of U.S. children (<48 months): findings from the Feeding Infants and Toddlers Study (FITS) 2016. J Nutr 2018; 148:1557S–1566S.
-
28 Denney L, Reidy KC, Eldridge AL: Differenc- es in complementary feeding of 6- to 23-month-olds in China, US and Mexico. J Nutr Health Food Sci 2016;4:1–8.
-
29 Afeiche MC, Koyratty BNS, Wang D, et al: Intakes and sources of total and added sugars among 4 to 13-year-old children in China, Mexico and the United States. Pediatr Obes 2018;13:204–212.
-
30 Wang D, van der Horst K, Jacquier EF, et al: Snacking patterns in children: a comparison between Australia, China, Mexico, and the USA. Nutrients 2018;10:198.