Early-Life Nutrition, Growth Trajectories, and Long-Term Outcome



Abstract
It is well established that nutrition during the first 1,000 days of life can have a long-term effect on growth, metabolic outcome, and long-term health. We review the long-term anthropometric follow-ups of children with risk of later morbidity: (a) very-low-birth- weight (VLBW) infants who have birth weights <10th percentile of weight and receive fortified breast milk, (b) infants from developing countries who are breastfed according to the present recommendations but have low birth weight and length, and (c) children from developed countries who were enrolled in randomized controlled trials (RCTs) to test if breastfeeding and low-protein formulas can prevent from rapid weight gain and childhood obesity. VLBW infants can be appropriate, small for gestational age (SGA), or intrauterine growth retarded (IUGR). SGA and IUGR (due to placenta insufficiency) infants are born with birth weights <10th percentile of weight for gestational age (GA). We pro- vided fortified breast milk until 52 weeks of GA to 31 SGA and 127 IUGR infants and fol- lowed up growth until 24 months. IUGR infants showed lower weight gain between birth and 3 months and had lower weight between 3 and 24 months (p < 0.05; ANCOVA). No significant BMI differences between SGA and IUGR infants were observed. It seems that IUGR infants receiving fortified breast milk need special attention, because without fur- ther improvement in breast milk fortification weight gain after discharge from hospital might be too slow. In developing countries, length and weight of breastfed infants during the first 2 years are strongly influenced by the respective anthropometric parameters at birth. Studies in the Gambia and Zimbabwe indicate that only breastfed infants with birth length and weight above the respective WHO 0 z-scores continue with adequate growth and have length and weight above the WHO 0 z-scores at 18 and 24 months. Prevalence of stunting and wasting in the overall Gambia breastfed infant population rapidly in- creases during the first year, peaks at around 3 years, but decreases thereafter. Long-term growth trajectories indicate later start of puberty and slow pubertal growth, but adult weight and height are not reached before 20–24 years. In adulthood, prevalence of stunting and wasting is much lower than during any period of childhood. Maternal risk factors, such as childhood marriage and poor nutrition before and during pregnancy, need to come into focus to improve birth length and weight and lower high stunting rates. Term breastfed infants from overweight/obese mothers and breastfed infants with rapid weight gain during infancy have increased risk of childhood obesity. Infants who are exclusively breastfed 4–6 months or receive low protein follow-up formulas (high-quality protein) grow slower during the first 2–3 years than infants fed high-protein formulas. During follow-up examinations at 5–6 years, they have lower BMI and obesity prevalence. Body composition measurements (DEXA) at 5–8 years in children who were breastfed and received low- or high-protein formula during infancy indicate that breastfeeding and feeding low-protein formulas are associated with lower gain of fat mass. Longitudinal cohort studies show that high-protein intake during the first 2 years results in higher BMI at 9 years and during adulthood. The studies presented indicate that breastfeeding but also other pre- and postnatal nutritional, epigenetic, and environmental factors influence growth trajectories and long-term health.
Introduction
It is well documented that maternal factors, events during the first 1,000 days of life, and early nutrition can have a long-term effect on growth, metabolic out- come, and long-term health [1, 2] (www.thousanddays.org). Growth of very- low-birth-weight (VLBW) infants (birth weight <1,500 g; gestational age [GA] <32 weeks) must be carefully monitored to avoid low postnatal weight gain that can be associated with a poor neurodevelopmental outcome [3, 4]. Faster weight gain on the other hand – the upward percentile crossing on a weight chart [5–7] – can be associated with childhood obesity and impaired metabolic out- come. We present growth trajectories of 2 cohorts of high-risk VLBW infants with birth weights <10th percentile for gestational age (GA) who received fortified breast milk until 52 weeks of GA.
Reviews of cross-sectional data from developing countries indicate that exclusive breastfeeding until 6 months helps to prevent from stunting, wasting, as well as from increased morbidity and mortality [8]. However, influences of maternal and intrauterine nutrition and complementary feedings that can be important for long-term growth and health have not been properly addressed. A long-term study in the Gambia [9] indicates that there might be windows of opportunity for nutritional intervention before and during pregnancy and after the first 1,000 days.
Breastfed infants in developed countries receive less protein than infants fed traditional infant/follow-up formulas [10]. Clinical trials indicate lower weight and body fatness in infants with lower protein intake [6, 11–13]. Long-term follow-up shows that higher protein intake during the first 12 months results in increased risk of overweight and obesity later in life [14]. To better understand long-term effects of early protein intake, we review indicators of body fatness and body composition in 5- to 8-year-old children who were breastfed or received formulas with different protein content.
Very-Low-Birth-Weight Infants
International pediatric societies still argue that postnatal growth of VLBW infants should be close to that of the in utero growing fetus. However, during postnatal adaption, extracellular water space is contracting, which results in 7–11% weight loss [15]; risks of morbidity and intolerance of enteral feeding are high, and neonatal intensive care (NICU) staff sometimes has to limit nutrient intake. VLBW infants (<1,500 g) reach their lowest weight between the 4th and 6th day of life, and birth weight is regained between 13 and 18 days of postnatal life [15]. After postnatal adaption, the new growth trajectories are parallel but approximately –0.8 z-scores below fetal growth standards [15]. Postnatal weight trajectories of VLBW infants who are born <10th percentile of weight for GA (“born too small”) are not so clear. For those VLBW infants, the terms small for GA (SGA) and intrauterine growth restriction (IUGR) are often synonymously used [16]. However, the underlying conditions that limit intrauterine growth are different: SGA represents a constitutionally small VLBW infant [17]. IUGR is a VLBW infant who fails to reach its potential growth due to maternal placental insufficiency, resulting in an impaired placental nutrient transport [18]. IUGR is a prenatal diagnosis, based on pathological ultrasound criteria according to the Clinical Guidelines of the Society of Maternal-Fetal Medicine [19]. In neonatal intensive care and during follow- up, all growth-restricted VLBW infants are treated the same, which includes nutritional management after birth: ESPGHAN recommends to apply an “enhanced nutrient strategy” after discharge from hospital up to the 52nd week of GA to all growth-restricted VLBW infants – preferably fortified human milk – regardless if they are SGA or IUGR [20]. Actually, reliable data proving that the recommended “enhanced nutrient strategy” is safe and effective both for VLBW infants who are SGA or IUGR are lacking, because most studies combined both groups in follow-up on growth. Epidemiological studies indicate that early nutrition during the pre- and postnatal life can have an impact on long-term health: undernutrition in utero permanently changes the body’s structure, function, and metabolism in ways that lead to obesity, insulin resistance, diabetes type 2, atherosclerosis, and associated cardiovascular ill-health later in life [1, 2, 21]. Postnatal centile crossing defined in terms of an upward change in weight z-score during 1 month [5–7; “rapid catchup growth”] in malnourished newborns can be associated with obesity and cardiovascular dis- eases in later life [22, 23]. In particular, it is not clear how IUGR infants react if they are exposed to prolonged postnatal exposure to an “enhanced nutrient concept.” Postnatal nutrition of all segments of VLBW infants must be safe, help to achieve optimal growth but also minimize the potential risk for later ill-health [23]. All VLBW infants in our NICU receive fortified breast milk until 52 weeks of corrected GA according to the present recommendations [20]. Long-term follow-up of postnatal growth of those infants is of interest to document their growth and development beyond infancy.
We investigated the impact of the “enhanced nutrient strategy” [18; ESPGHAN] on anthropometric parameters of all SGA and IUGR VLBW infants who were treated in our NICU during the last decade and could be followed up until 2 years in our outpatient clinic. All study infants had pre- and postnatal examinations in regular intervals: 31 SGA infants without genetic defects or malformations and 127 IUGR infants with intrauterine pathological ultrasound pattern [19]. Median birth weights of SGA and IUGR were 600 and 688 g (nonsignificant), and median GAs were 25 weeks (+6 days) and 29 weeks (+1 day; p < 0.001), respectively [24]. Enteral feedings of all infants started with breast milk that was then fortified with a human milk fortifier to increase protein, caloric, and micronutrient concentrations of feedings. At discharge, 68% of the infants exclusively received fortified breast milk [24].
Weight gain of IUGR infants was lower between birth and 3 months with a change from –1 to –2 WHO z-scores (Fig. 1). Poor weight gain was mainly ob- served after discharge from hospital. This resulted in significantly lower weight of IUGR infants between 3 and 24 months (corrected for sex and GA; ANCOVA). SGA and IUGR infants gained 1.3 and 1.7 z-score points between 3 and 24 months corrected for GA. Mean weight of SGA infants crossed the 10th percentile of the WHO standards (http://www.who.int/childgrowth/standards/en/) at 6 months, whereas weight of IUGR infants remained below the 10th percentile until 24 months. Standard deviations indicate that until 24 months some infants would be still classified as malnourished, because their weight was below –2 z-scores of the WHO charts. Both groups did not show upwards crossing of percentiles during 1 month [7], that is, no accelerated weight gain until 24 months.
BMI of both groups did not deteriorate between birth and 3 months. Between 3 and 24 months, no significant BMI differences between SGA and IUGR infants were observed. SGA and IUGR infants gained 0.6 and 0.8 z-score points between 3 and 24 months (Fig. 2).Our preliminary data indicate lower weight gain of IUGR infants during the period when the enhanced nutrient strategy [20] is applied. This results in lower weight until 24 months. To answer the question if there is a need to develop separate nutrition guidelines for VLBW infants who are SGA or IUGR, randomized controlled studies (RCTs) with further improved breast milk fortification which include anthropometry, body composition, epigenetic, metabolic, and neurodevelopmental outcomes, and the microbiome are necessary.
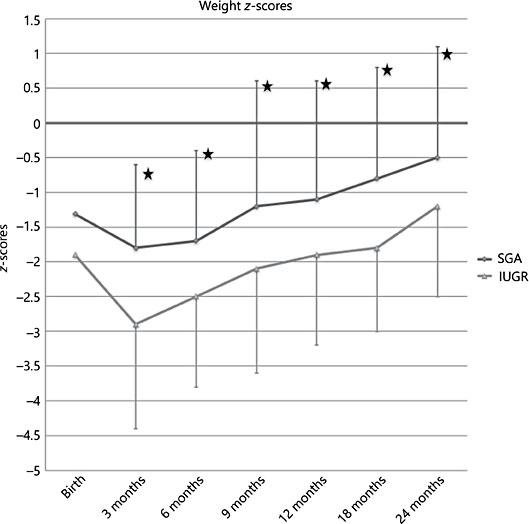
Fig. 1. Weight z-scores (x, SD) of SGA- and IUGR VLBW infants at birth and from 3 to 24 months (corrected for prematurity). Weight reference at birth: http://www.merckmanuals.com/en-ca/professional/pediatrics/perinatal-prob. Weight standard from 3 to 24 months: http://www.who.int/childgrowth/standards/en/. Analysis: ANCOVA with birth- weight and sex as covariates. * p < 0.05.
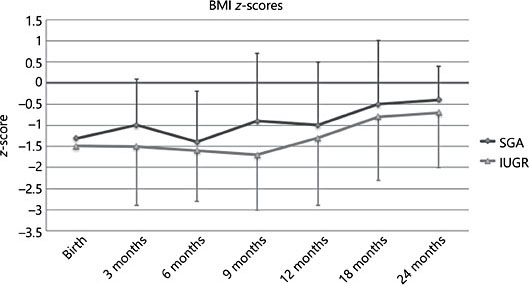
Fig. 2. BMI z-scores (x, SD) of SGA- and IUGR VLBW infants at birth and from 3 to 24 months (corrected for prematurity). BMI reference at birth: http://www.merckmanuals.com/en- ca/professional/pediatrics/perinatal-prob. BMI standard from 3 to 24 months: http:// www.who.int/childgrowth/standards/en/.
Breastfed Infants from Developing Countries – Stunting
Before a child’s 6th birthday, the brain matures more rapidly than at any other time in life. Poor nutrition can have a profound, lifelong impact on a child’s growth, learning, and health. In 2018, WHO, UNICEF, and the World Bank (WHO/UNICEF) report that the number of children (<5 years) who are stunted has worldwide declined from approximately 250 million (1990) to 150 million (2015), but the number of stunted children increased in sub-Saharan Africa from 45 to 57 million in 2015. Therefore, it seems unlikely that the global WHO targets 2025 to reduce stunting by 40% will be met in sub-Saharan Africa during the next decade. Exclusive breastfeeding plays a key role in the prevention of stunting and wasting: the associations of breastfeeding with growth and health in developing countries can be studied by repeatedly analyzing demographic health surveys (DHS; US) data sets that provide information on nutrition, growth, and health. We reviewed data of more than 130,000 infants and small children (0–6, 6–12, and 12–24 months) from 20 developing countries that were collected at least twice in intervals of 5–10 years during the last 2 decades [8; unpubl. data]. Our sample (Table 1) indicates an exclusive breastfeeding rate of 32% (96% overall breastfeeding rate) during the first 6 months and is therefore representative for all developing countries, where WHO estimates the respective exclusive breastfeeding rate to be about 34%.
Table 1 shows growth and health of infants who are exclusively or not exclusively breastfed, or not breastfed. Prevalence of stunting and wasting was already high during the first 6 months. Exclusive breastfeeding was associated with significantly higher weight, length, and lower probability of stunting, wasting, and infections. Between 6 and 12 months when 90% of infants were still breastfed and stunting and wasting, prevalence was already 24 and 11%, respectively; the association of breastfeeding with lower prevalence of stunting and wasting was no more present, but the probability of infections tended to be lower [8]. Be- tween 12 and 24 months, when stunting (45%) and wasting prevalence (14%) was very high, 74% of the infants still received breast milk. During the second year of life, breastfeeding was associated with significantly higher stunting and wasting prevalence [8]. DHS data are cross-sectional and indicate associations and no causal relationships. Like many other studies, they underline the importance of exclusive breastfeeding for growth and health during the first 6 months, but a recent well-controlled longitudinal cohort study in the Gambia (n = 756) challenges that exclusive breastfeeding improves length for age z-scores at 6, 12, and 24 months [25]. DHS data of infants between 6 and 24 months also reflect the influence of low-quality complementary feedings and poor environmental conditions in developing countries, which contribute to the high stunting and wasting rates. A systematic review of trials in developing countries which provide complementary foods and education [26] showed significant effect sizes of +0.17 for length/height for age z-scores and +0.35 for weight/age z-scores. Similar effects were found when energy density of the usual complementary foods was increased.
Victora et al. [27] showed that in poor regions of the world, such as Southeast Asia and Africa, growth is already disturbed during the embryonic and fetal period. Average height/age z-scores (HAZ) at birth were –0.75 and –0.35 and further declined during the first 2 years by approximately 1.5 HAZ. No detailed data on feeding mode were included. Growth trajectories from 2 well-controlled African cohorts [28; unpubl. data provided to the authors; 29, 30] with strong breastfeeding support showed the importance of maternal stature, nutrition, and health, as well as maternal nutrition before conception and during pregnancy: growth trajectories of infants who were in the top 10th percentile segment of length at birth grew almost according to the WHO standards until 2 years. However, those infants in the bottom 10th percentile segment at birth (i.e., newborns with disturbed intrauterine growth) showed poor growth and had mean length at 2 years that was below the –2 z-score of the WHO standards. In addition to breastfeeding support, future key targets should be to improve nutrition of adolescent girls, young women, and during pregnancy, but studies with targeted interventions are still lacking [31–33].
Timing of cell-proliferative potential of organ systems across childhood and adolescence does not support the concept of a catchup window closing at 24 months [28]. Analysis of data from various sources shows that catchup in height z-scores occurs after 24 months in many poor populations, even in the absence of interventions: early height growth in 5 populations (Brazil, Guatemala, India, Philippines, and South Africa), each studied longitudinally and brought together in the COHORTS collaboration [34], confirmed the rapid fall- off in height z-scores between birth and 24 months in all 5 countries, but also showed significant regain between 24 and 48 months in 4 of the 5 cohorts. Both the falloff and catchup was observed irrespective of the final height attained. India was a distinct outlier with no signs of catchup. Prentice et al. [28] showed that in children from rural Gambia who were breastfed substantial height catch- up occurred between 24 months and childhood and again between childhood and adulthood, even in the absence of any interventions. Development of better adaptive response mechanisms against pathogens might reduce the frequency and severity of growth-limiting infections. Longitudinal growth data from that country illustrate that an extended pubertal growth phase allows very considerable height recovery, especially in girls during adolescence. In light of the critical importance of maternal stature to her children’s health, it becomes clear that adolescence represents an additional window of opportunity during which sub- stantial life cycle and intergenerational effects can be accrued.
The traditional view has been that the “window of opportunities” for growth- and health-promoting interventions should the period between the day of conception and 24 months (“first 1,000 days”; www.thousanddays.org). Interventions before the first 1,000 days have only been recently in focus of scientific research [28, 31–34]. Epigenetically mediated early-life and/or intergenerational effects may also contribute to population diversity in later growth [28]. Height catchup in young children, even in the absence of external nutritional interventions, clearly contradicts the widely held impression that a window of opportunity closes at 24 months of age [9]. The extent of catchup after 24 months is highly context specific and presumably reflects the availability of foods, food consumption patterns, the composition of diets, and the prevailing burden of infections (especially those affecting gastrointestinal function).
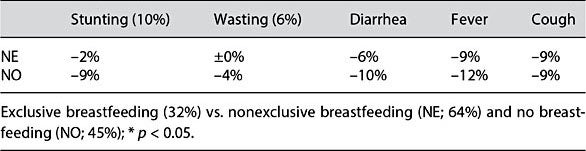
Table 1. Comparison of growth and health of infants (0–6 months) from 20 developing countries
Is Low Protein Intake during the Breastfeeding Period and Beyond a Factor That Contributes to Obesity Prevention?
Term breastfed infants from overweight/obese mothers and breastfed infants with rapid weight gain during infancy have an increased risk of obesity during childhood, adolescence, and adulthood, which can be associated with disturbed metabolic outcome and higher risk of diabetes and cardiovascular dis- ease [35–37]. Dewey at al. [38] compared weight, length, and weight-for- length ratios of infants who were breastfed or fed infant formulas and found that breastfed infants are leaner. Energy intake of breastfed infants at 3 and 6 months was 13–20% lower, but protein intake was 43–47% lower [39]. Formulas in the Darling study [39] had higher protein concentrations than modern formulas which have been on the markets during the last 10 years. It was suggested that higher protein intake could be the reason for “accelerated growth” in formula-fed infants [39], which could be a risk factor later in life. Differences in growth between breast- and formula-fed infants are one of the reasons why the WHO (http://www.who.int/childgrowth/standards/en/) start- ed to collect data to construct the WHO growth standards, which are based on infants who were predominately breastfed at least for 4–6 months and where breastfeeding continued beyond 6 months. It must be pointed out that until now there are no randomized trials which compare long-term growth of exclusively breastfed (i.e., 4–6 months) and formula infants. For obvious reasons, it is most unlikely that such trials will be conducted in the future. PROBIT in Belarus [40] is the only randomized cluster intervention trial that looks at feeding modes during the first 6 months and long-term growth. A breastfeeding intervention group (modeled by the WHO/UNICEF baby-friendly hospital initiative) was compared with a group without any intervention. Exclusive breastfeeding rates at 3 months in the intervention and control groups were 43.3 and 6.4% (p < 0.001). Corresponding rates at 6 months were as low as 7.9 and 0.6%. No differences in growth and adiposity between groups were found at 6.5 and 11.5 years [41]. Because of the low percentages of breastfed infants in the intervention group at 3 and 6 months, the PROBIT study cannot answer the question if exclusive breastfeeding according to the international recommendations (4–6 months) helps to lower the prevalence of childhood obesity in developed countries.
RCTs that compare and follow up growth of appropriate- or SGA term newborns [6, 11–13] can help to answer the question: infants were exclusively breastfed for 3–6 months or received low- or high-protein formulas until 9 or 12 months of age. Caloric density of higher- and lower-protein formulas was almost equal in three trials [11–13], whereas in one trial the high-protein formula had a 6% higher energy density [6]. During and/or at the end of the intervention, all studies showed lower weight in the breastfed and low-protein formula groups than in the high-protein formula groups (Table 2) [11–13, 26]. Follow-up at 2 [11, 12] and 3 years [12] indicated lower weight and BMI in the breastfed and low-protein formula groups. The breastfed group in the multicenter US study [13] at 5 years still had lower weight (–853 g; 95% CI 12.9–1,695.0; p ≤ 0.047) and BMI (–0.56; 95% CI 0.09–1.02; p ≤ 0.021) than the high-protein formula group. Differences between the breastfed and low-protein formula group were small and not significant. At 6 years, the European multicenter CHOP study [11, 14] reported significantly lower BMI and lower percentage of obesity in the breastfed and the low- than in the high-protein formula group.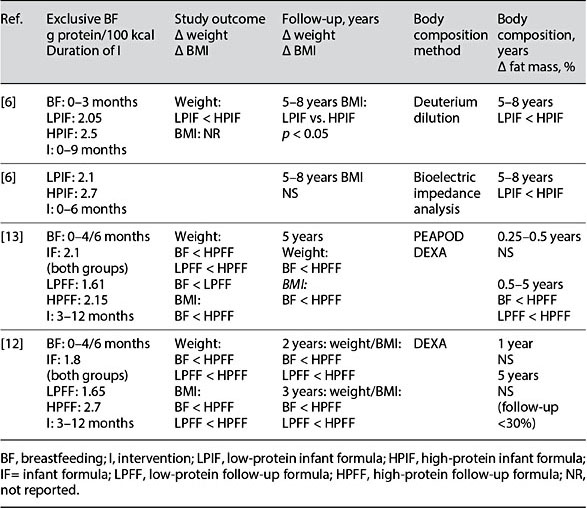
Table 2. RCTs. Protein intake during infancy, growth, and body composition
Body Composition
A long-term follow-up of 4 RCTs with body composition measurements be- tween 5 and 8 years has been published: Singhal et al. [6] compared fat mass (kg) of children with birth weights <10th percentile (weight) who were exclusively breastfed or received a low-or high-protein formula (Table 2). Unadjusted body fat mass was about 40 and 26% lower [6] in the breastfed and low- protein formula groups than in the high-protein formula group. Gender-adjusted differences between the low- and high-protein group were highly significant (p < 0.009). In another study [9], children with birth weights <20th percentile (weight) were fed a low- or high-protein formula until 6 months. The high-protein formula provided 12% more calories per 100 ml. No breast- fed group was included. In the low-protein formula group, fat mass at 5–8 years was 18% lower. When confounders were considered, the difference be- came significant (p ≤ 0.04). In a subsample of a US multicenter RCT [13], longitudinal changes in body composition between 6 and 60 months of age have been documented. [37]. References [42] indicate that children during this period are becoming about 10% leaner. In the US study [13, 37], percent body fat decreased 7.3, 4.9, or 2.0%, in children who were exclusively breastfed or received low- or high-protein formula, respectively. Differences between the breastfed and low-protein formula group on the one hand and the higher- protein group on the other hand were statistically significant (p < 0.05) [37]. One RCT in children from overweight mothers [12, 37] did not show differences in body composition but had poor follow-up of DEXA measurements at 5 years (<30%).
Cohort Studies
Two longitudinal cohort studies support the findings from RCTs that low protein intake during early life with breast milk or low-protein formula is associated with a lower obesity risk later in life. Braun et al. [43] reported that in a Dutch cohort lower protein intake at 12 months was associated with lower weight and BMI at 9 years. In the same cohort, lower protein intake and slower weight gain during infancy was associated with lower fat mass (DEXA) and lower BMI at 6 years [44]. Rolland-Cachera [45] showed that in a cohort which represented the French childhood population, lower protein intake during the first 2 years was associated with significantly lower BMI at 20 years.
It is evident that low protein intake with breast milk can contribute to later obesity prevention. The effect size has been estimated to be as high as 20% [6]. RCTs show that low-protein formulas can contribute to obesity prevention if breastfeeding is not possible or too short. It seems that the second half of the first year and the second year are more critical because present follow-up formulas and cow’s milk provide 2.5 and 4 times more protein than breast milk [10]. EFSA, the European Food Safety Agency, recently approved follow-up formulas with 1.6 g protein per 100 kcal if clinical trials prove safety.
Conclusions
VLBW infants who are IUGR show low weight gain after discharge from hospital when they receive fortified breast milk. RCTs are necessary to confirm the results of our cohort study and to test new fortification strategies of breast milk. Stunting rates in children from developing countries are still high. Exclusive breastfeeding is important to prevent infants from stunting. Further preventive measures include nutritional supplementation of young women before and during pregnancy, promotion of breastfeeding and improvement of quality of complementary foods. RCTs which include follow-up of growth and body composition during childhood indicate that breastfeeding and the use of low-protein formulas can contribute to the prevention of rapid weight gain during infancy and childhood obesity.
References
- 1 Barker DJ, Gluckman PD, Godfrey KM, et al: Fetal nutrition and cardiovascular disease in adult life. Lancet 1993;341:938–941.
- 2 Godfrey KM, Costello PM, Lillycrop KA: Development, Epigenetics and Metabolic Programming. Nestle Nutr Inst Workshop Ser 2016;85:71–80.
- 3 Belfort MB, Ehrenkranz RA: Neurodevelopmental outcomes and nutritional strategies in very low birth weight infants. Semin Fetal Neonatal Med 2017;22:42–48.
- 4 Castanys-Muñoz E, Kennedy K, Castañeda- Gutiérrez E, et al: Systematic review indicates postnatal growth in term infants born small- for-gestational-age being associated with later neurocognitive and metabolic outcomes. Acta Paediatr 2017;106:1230–1238.
- 5 Fewtrell MS, Morley R, Abbott RA, et al: Catch-up growth in small-for-gestational-age term infants: a randomized trial. Am J Clin Nutr 2001;74:516–523.
- 6 Singhal A, Kennedy K, Lanigan J, et al: Nutrition in infancy and long-term risk of obesity: evidence from 2 randomized controlled trials. Am J Clin Nutr 2010;92:1133–1144.
- 7 Cole TJ, Singhal A, Fewtrell MS, et al: Weight centile crossing in infancy: correlations between successive months show evidence of growth feedback and an infant-child growth transition. Am J Clin Nutr 2016;104:1101–1109.
- 8 Haschke F, Haiden N, Detzel P, et al: Feeding patterns during the first 2 years and health outcome. Ann Nutr Metab 2013;62(suppl 3):16–25.
- 9 Prentice AM, Ward KA, Goldberg GR, et al: Critical windows for nutritional interventions against stunting. Am J Clin Nutr 2013; 97:911–918.
- 10 Haschke F, Haiden N, Thakkar SK: Nutritive and bioactive proteins in breastmilk. Ann Nutr Metab 2016;69(suppl 2):17–26.
- 11 Koletzko B, von Kries R, Closa R, et al: Lower protein in infant formula is associated with lower weight up to age 2 years: a randomized clinical trial. Am J Clin Nutr 2009;89:1836– 1845.
- 12 Inostroza J, Haschke F, Steenhout P, at al: Low-protein formula slows weight gain in infants of overweight mothers. J Pediatr Gas- troenterol Nutr 2014;59:70–77.
- 13 Ziegler EE, Fields DA, Chernausek SD, et al: Adequacy of infant formula with protein content of 1.6 g/100 kcal for infants between 3 and 12 months. J Pediatr Gastroenterol Nutr 2015;61:596–603.
- 14 Weber M, Grote V, Closa-Monasterolo, et al: Lower protein content in infant formula reduces BMI and obesity risk at school age: follow-up of a randomized trial. Am J Clin Nutr 2014;99:1041–1051.
- 15 Rochow N, Raja P, Liu K, et al: Physiological adjustment to postnatal growth trajectories in healthy preterm infants. Pediatr Res 2016;79: 870–879.
- 16 Harkness UF, Mari G: Diagnosis and management of intrauterine growth restriction. Clin Perinatol 2004;31:743–764.
- 17 American College of Obstetricians and Gynecologists: ACOG Practice bulletin No. 134: fetal growth restriction. Obstet Gynecol 2013; 121:1122–1133.
- 18 Baschat AA: Pathophysiology of fetal growth restriction: implications for diagnosis and surveillance. Obstet Gynecol Surv 2004;59: 617–627.
- 19 Society for Maternal-Fetal Medicine Publications Committee, Berkley E, Chauhan SP, Abuhamad A: Doppler assessment of the fetus with intrauterine growth restriction. Am J Obstet Gynecol 2012;206:300–308.
- 20 ESPGHAN Committee on Nutrition, Aggett PJ, Agostoni C, et al: Feeding preterm infants after hospital discharge: a commentary by the ESPGHAN Committee on Nutrition. J Pedi- atr Gastroenterol Nutr 2006;42:596–603.
- 21 Okada T, Takahashi S, Nagano N, et al: Early postnatal alteration of body composition in preterm and small-for-gestational-age infants: implications of catch-up fat. Pediatr Res 2015;77:136–142.
- 22 Neitzke U, Harder T, Plagemann A: Intra- uterine growth restriction and developmental programming of the metabolic syndrome: a critical appraisal. Microcirculation 2011;18: 304–311.
- 23 Lafeber HN, van de Lagemaat M, Rotteveel J, van Weissenbruch M: Timing of nutritional interventions in very-low-birth-weight infants: optimal neurodevelopment compared with the onset of the metabolic syndrome. Am J Clin Nutr 2013;98:556S–560S.
- 24 Huber-Dangl M: Growth and Neurodevelopmental Outcome in Very-Low Birthweight Infants Who Are Small for Gestational Age or Intrauterine Growth Retarded (IUGR) – A Retrospective Analysis; Diploma thesis. Medical University of Vienna, Vienna, 2017.
- 25 Eriksen KG, Johnson W, Sonko B, et al: Following the World Health Organization’s recommendation of exclusive breastfeeding to 6 months of age does not impact the growth of rural Gambian infants. J Nutr 2017;147:248– 255.
- 26 Dewey KG, Adu-Afarwuah S: Systematic re- view of the efficacy and effectiveness of complementary feeding interventions in developing countries. Matern Child Nutr 2008; 4(suppl 1):24–85.
- 27 Victora CG, de Onis M, Hallal PC, et al: Worldwide timing of growth faltering: revisiting implications for interventions. Pediatrics 2010;125:e473–e480.
- 28 Prentice AM, Ward KA, Goldberg GR, et al: Critical windows for nutritional interventions against stunting. Am J Clin Nutr 2013; 97:911–918.
- 29 Prendergast AJ, Humphrey JH: Stunting Persists despite Optimal Feeding: Are Toilets Part of the Solution? Nestle Nutr Inst Work- shop Ser 2015;81:99–110.
- 30 Gough EK, Moodie EE, Prendergast AJ, et al: Linear growth trajectories in Zimbabwean infants. Am J Clin Nutr 2016;104:1616–1627.
- 31 Krebs N, Bagby S, Bhutta ZA, et al: International summit on the nutrition of adolescent girls and young women: consensus statement. Ann NY Acad Sci 2017;1400:3–7.
- 32 Lassi ZS, Moin A, Das JK, et al: Systematic review on evidence-based adolescent nutrition interventions. Ann NY Acad Sci 2017; 1393:34–50.
- 33 Lassi ZS, Mansoor T, Salam RA, et al: Review of nutrition guidelines relevant for adolescents in low- and middle-income countries. Ann NY Acad Sci 2017;1393:51–60.
- 34 Stein AD, Wang M, Martorell R, et al; Cohorts Group: Growth patterns in early child- hood and final attained stature: data from five birth cohorts from low- and middle-in- come countries. Am J Hum Biol 2010;22: 353–359.
- 35 Godfrey KM, Reynolds RM, Prescott SL, et al: Influence of maternal obesity on the long- term health of offspring. Lancet Diabetes Endocrinol 2017;5:53–64.
- 36 Lin X, Lim IY, Wu Y, et al; GUSTO Study Group: Developmental pathways to adiposity begin before birth and are influenced by genotype, prenatal environment and epigenome. BMC Med 2017;15:50.
- 37 Haschke F, Gratwohl D, Haiden N: Metabolic Programming: Effects of Early Nutrition on Growth, Metabolism and Body Composition. Nestlé Nutr Inst Workshop Ser 2016;86:87– 95.
- 38 Dewey KG, Heinig MJ, Nommsen LA, et al: Breast-fed infants are leaner than formula-fed infants at 1 y of age: the DARLING study. Am J Clin Nutr 1993;57:140–145.
- 39 Heinig MJ, Nommsen LA, Peerson JM, et al: Energy and protein intakes of breast-fed and formula-fed infants during the first year of life and their association with growth veloc- ity: the DARLING Study. Am J Clin Nutr 1993;58:152–161.
- 40 Kramer MS, Chalmers B, Hodnett ED, et al; PROBIT Study Group: Promotion of Breast- feeding Intervention Trial: a randomized trial in the Republic of Belarus. JAMA 2001;285: 413–420.
- 41 Martin RM, Patel R, Kramer MS, et al: Effects of promoting longer-term and exclusive breastfeeding on adiposity and insulin-like growth factor-I at age 11.5 years: a randomized trial. JAMA 2013;309:1005–1013.
- 42 Fomon SJ, Haschke F, Ziegler EE, Nelson SE: Body composition of reference children from birth to age 10 years. Am J Clin Nutr 1982; 35(5 suppl):1169–1175.
- 43 Braun KV, Erler NS, Kiefte-de Jong JC, et al: Dietary intake of protein in early childhood is associated with growth trajectories between 1 and 9 years of age. J Nutr 2016;146:2361– 2367.
- 44 Voortman T, Braun KV, Kiefte-de Jong JC, et al: Protein intake in early childhood and body composition at the age of 6 years: the Generation R Study. Int J Obes 2016;40:1018–1025.
- 45 Rolland-Cachera MF, Akrout M, Péneau S: Nutrient intakes in early life and risk of obe- sity. Int J Environ Res Public Health 2016; 13:E564.