Dietary Carbohydrates and Childhood Functional Abdominal Pain
59 min read
Key insights
Childhood AP-FGIDs affect up to 20% of children worldwide. These disorders are now classified as irritable bowel syndrome (IBS), functional dyspepsia, functional abdominal pain, and abdominal migraine. Many potential factors have been linked to AP-FGIDs, including psychosocial stress, inflammation, and alterations in gut homeostasis and function. The role of diet is particularly relevant, as the symptoms of AP-FGIDs are associated with intake of certain foods.
Current knowledge
Childhood AP-FGIDs affect up to 20% of children worldwide. These disorders are now classified as irritable bowel syndrome (IBS), functional dyspepsia, functional abdominal pain, and abdominal migraine. Many potential factors have been linked to AP-FGIDs, including psychosocial stress, inflammation, and alterations in gut homeostasis and function. The role of diet is particularly relevant, as the symptoms of AP-FGIDs are associated with intake of certain foods.
Practical implications
Each individual malabsorbed carbohydrate (i.e. lactose or fructose) exerts distinct physiological effects. Other factors which may affect symptom severity include the presence of low-grade gut inflammation and visceral hypersensitivity. Dietary restriction of FODMAP carbohydrates is a potential strategy for mitigating gastrointestinal symptoms in childhood IBS. Data from randomized controlled trials also indicate that soluble fiber supplementation can reduce abdominal pain in children with AP-FGIDs.
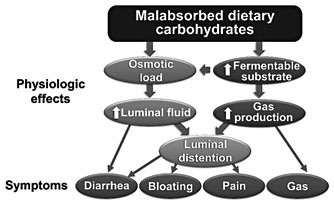
Carbohydrate malabsorption may cause gastrointestinal symptoms (e.g., bloating) via the physiologic effects of both increased osmotic activity and increased gas production from bacterial fermentation.
There is a general lack of strong evidence supporting a restriction of individual carbohydrates (e.g., lactose) for childhood functional gastrointestinal disorders; however, emerging evidence suggests that a restriction of fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) may be effective.
Soluble fiber (a complex carbohydrate) supplementation via randomized controlled intervention trials in childhood functional gastrointestinal disorders has demonstrated efficacy.
Childhood abdominal pain-related functional gastrointestinal disorders (AP-FGIDs) affect up to 20% of children worldwide and account for at least 5% of all pediatric office visits in the United States [1, 2]. These disorders do not have an identifiable organic etiology based on conventional diagnostic testing; nevertheless, children with AP-FGIDs have both decreased quality of life and increased school absences as compared to their peers [3]. The gastrointestinal (GI) symptoms (e.g., abdominal pain) associated with these disorders may persist for years and into adulthood [4]. Successful interventions that ameliorate these symptoms in childhood AP-FGIDs may have an impact into adulthood [4]. Unfortunately, despite growing interest and research, current conventional clinical interventions for these disorders are often ineffective.
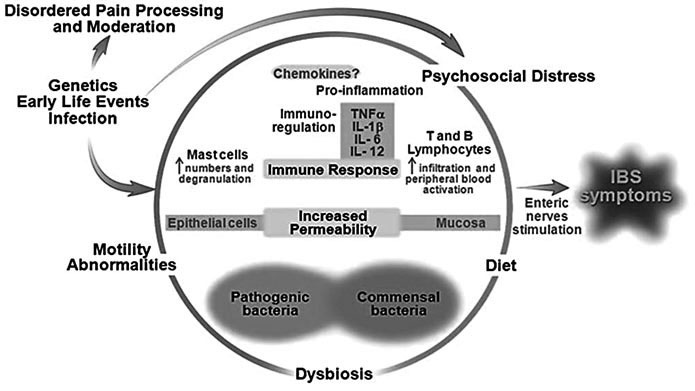
Though previously defined under the broad category of recurrent abdominal pain (RAP), using Rome III criteria, AP-FGIDs are now classified into: irritable bowel syndrome (IBS), functional dyspepsia, functional abdominal pain, and abdominal migraine [5]. The etiology of AP-FGIDs is believed to be multifactorial and is best approached using the biopsychosocial model (fig. 1). Potential factors include: psychosocial distress (e.g., somatization, anxiety); alterations in the composition and function of the gut microbiome; low-grade gut inflammation; increased gut permeability; visceral hypersensitivity; altered GI motor function, and diet. Diet in particular has generated interest as a culprit given that children with AP-FGIDs often associate symptoms with intake of particular foods [6].
Fig. 1. Biopsychosocial model of FGIDs. Modified from Rodriguez-Fandino et al. [45] with permission from the Journal of Neurogastroenterology and Motility.
Carbohydrates provide the majority of calories consumed in the Western diet [7]. For many decades, individual carbohydrates (e.g., lactose) have been implicated both as culprits for the etiology of symptoms and as potential therapeutic agents (e.g., fiber) in children with APFGIDs. This review will examine the proposed pathophysiology of carbohydrate intolerance and the current evidence implicating individual carbohydrates and groupings of carbohydrates in causing or improving symptoms in childhood AP-FGIDs. It will also briefly examine the proposed digestive physiology of fiber and the current evidence pointing toward the use of fiber in children with AP-FGIDs.
Carbohydrate Intolerance
Proposed Common Pathophysiologic Mechanisms
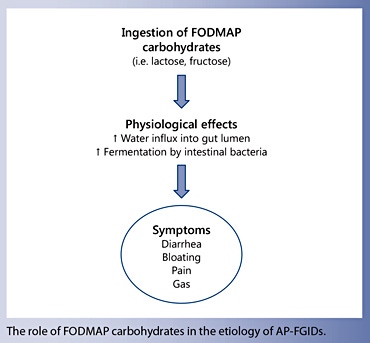
In children with AP-FGIDs, several individual carbohydrates (including lactose and fructose) have been implicated as exacerbating GI symptoms [8, 9]. As a group, these individual carbohydrates in combination with fructans, galactans, and polyols are termed fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) carbohydrates ( table 1 ). FODMAP carbohydrates are rapidly fermented by colonic bacteria and are osmotically active ( fig. 2 ). These physiologic effects can cause colonic distention from influx of water into the lumen and may lead to symptoms of abdominal pain, flatus, bloating, and loose and/or more frequent stools. These nonimmunologic adverse reactions to carbohydrates are termed carbohydrate intolerance.
Fig. 2. Proposed pathophysiologic mechanism of malabsorbed carbohydrates in FGIDs. Modified from Barrett et al. [46] with permission from Practical Gastroenterology.
Though grouped together as FODMAP carbohydrates, each individual malabsorbed carbohydrate may have a different physiologic effect. Magnetic resonance imaging evaluation in healthy adults demonstrates that fructose significantly increases small bowel water content; however, fructans increase small bowel water content to a much smaller degree [10]. In comparison, fructans significantly distend the colonic lumen; however, fructose increases colonic distention to a much smaller degree [10]. The individual effects of lactose, galactans, and polyols on GI physiologic function as measured by magnetic resonance imaging remain to be elucidated. In addition, whether these same physiologic changes occur following FODMAP carbohydrate ingestion in children (or adults) with AP-FGIDs is unknown.
Additional factors which may play a role in the generation of symptoms in subjects with lactose intolerance include low-grade gut inflammation and visceral hypersensitivity [11]. This was demonstrated by Yang et al. [11] in adults with IBS following lactose challenge and breath hydrogen testing to identify lactose malabsorbers (increased hydrogen production following the lactose challenge). Those with IBS who had lactose malabsorption were categorized into one of two groups: lactose malabsorption with lactose intolerance (concomitant increase in GI symptoms with the lactose challenge) and lactose malabsorption without lactose intolerance (no increase in GI symptoms). Yang et al. [11] found that adults with IBS with lactose malabsorption and intolerance (in comparison to those with malabsorption alone) had both increased mast cells in ileocolonic biopsies and increased visceral hypersensitivity. Whether these factors also play a role in carbohydrate intolerance in childhood AP-FGIDs is currently unknown.
Lactose
Hippocrates first described lactose intolerance around 400 years BC, but the clinical symptoms have only become recognized in the past 50 years [12]. Lactose is a disaccharide (two conjoined sugars) that is unique in that it is only present in mammalian milk with estimates of 5.5–8.0 g/100 ml in human breast milk and 4.5– 5.0 g/100 ml in cow’s milk [13] . In order to be utilized, lactose needs to be broken down (hydrolyzed) by the enzyme lactase. Lactase is found on the tips of the villi of the small intestine and breaks down lactose into two monosaccharides – galactose and glucose. These monosaccharides are then absorbed by the small intestine and metabolized.
At the time of birth in humans, lactase activity is at its peak. However, lactase activity begins to decrease in early childhood in approximately 70% of humans; by adulthood, lactase activity is very low or undetectable [14, 15]. Approximately 30% of the population has lactase persistence whereby lactase activity remains beyond weaning and into adulthood [14, 15]. Lactase persistence occurs primarily in people of northern European descent.
The amount of lactose needed to induce symptoms in someone who is lactose intolerant varies depending on numerous factors. These include: (1) the amount of lactose ingested; (2) whether ingestion is accompanied by a meal or other food; (3) the rate of gastric emptying (how quickly the meal enters the small intestine); (4) small intestinal transit time (the time it takes for a meal to enter the large intestine after first entering the small intestine); (5) whether the meal contains bacteria with enzymes (beta- galactosidase) capable of breaking down lactase, and (6) colonic bacterial adaptation to one’s previous diet [16, 17]. For example, in one study, single lactose loads of ≥ 15 g produced symptoms in the majority of lactase-deficient adults; however, lactose loads of up to 12 g (particularly if spread throughout the day) resulted in minimal or no symptoms [18]. Similarly, feeding subjects dairy-based yogurts with viable microbial cultures that contain bacteria with beta-galactosidase activity resulted in fewer signs of lactose malabsorption than feeding them pasteurized yogurts with little beta-galactosidase activity [17]. The amount of lactose needed to induce symptoms in a child with lactose malabsorption (either healthy or with an AP-FGID) is currently unknown.
Two other studies support a dose-response gradient of lactose exposure and symptoms. One study challenged 13 healthy adults with lactose maldigestion with varying amounts of lactose (0, 2, 6, 12, and 20 g) [16]. This study found that doses of up to 6 g (representing 120 ml of milk) were well tolerated, but symptoms began to emerge at 12 g of exposure [16]. Similar findings were noted in adults challenged with increasing quantities of lactose in a lactose-hydrolyzed milk preparation; the severity of symptoms was primarily dependent on the amount of lactose present [19].
Lactose-Related Studies in Children with AP-FGIDs
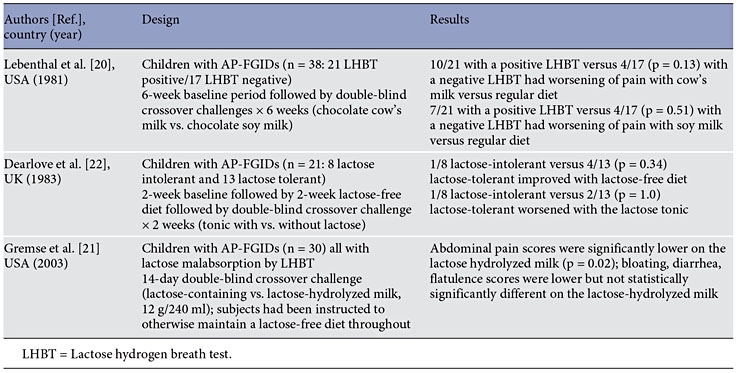
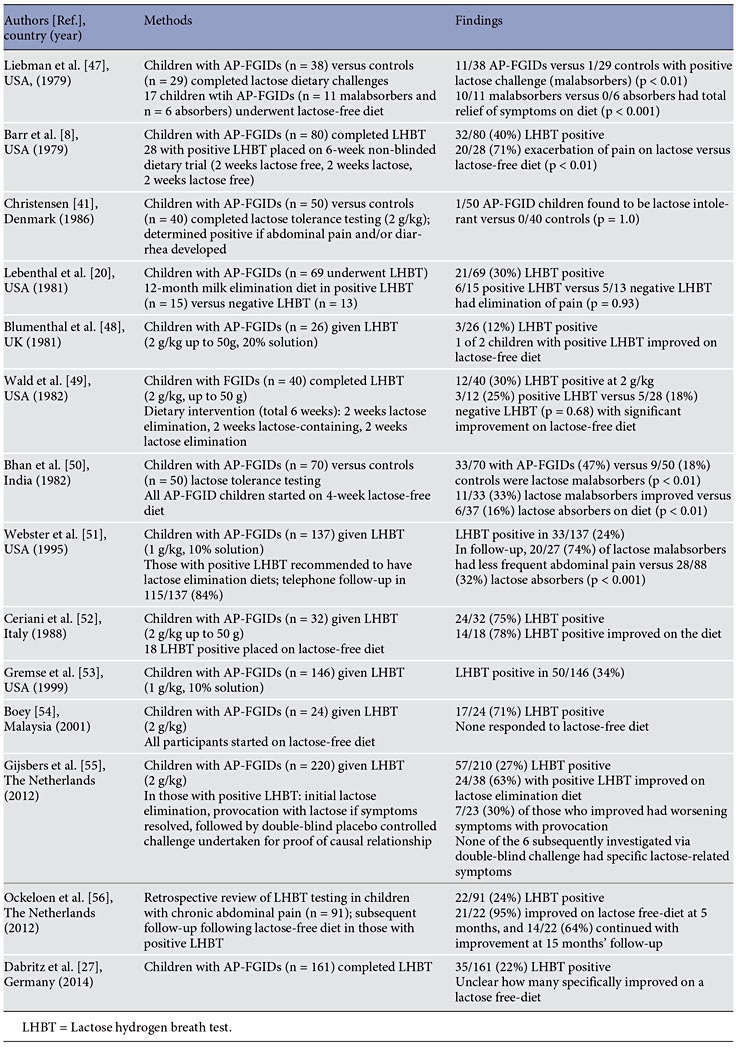
In children with AP-FGIDs, three randomized controlled trials have been completed, though none evaluated a restricted lactose diet in a controlled fashion ( table 2 ). There have been a greater number of observational or uncontrolled trials ( table 3 ). Lebenthal et al. [20] used both a randomized controlled challenge and an uncontrolled treatment component. The majority of the trials employed either: a lactose challenge (to identify those who were lactose intolerant based on the development of GI symptoms); or a lactose hydrogen breath test (to identify children who were malabsorbing lactose by demonstrating an excessive amount of hydrogen production within a specified time after lactose ingestion).
Table 2. Prospective randomized controlled trials of lactose in children with AP-FGIDs
Table 3. Observational or uncontrolled lactose-related studies in children with AP-FGIDs
The randomized controlled trials provide mixed results regarding the ability of lactose to worsen symptoms in children with AP-FGIDs. One trial identified worsening abdominal pain (but not other symptoms) in children with AP-FGIDs with lactose malabsorption when using nonhydrolyzed lactose milk versus hydrolyzed lactose milk [21]. However, the other two trials did not find that lactose significantly worsened symptoms in children with AP-FGIDs and lactose malabsorption [20, 22]. Similarly, the uncontrolled studies have had mixed results with respect to both the proportion of children with AP-FGIDs who have lactose malabsorption and the efficacy of a lowlactose diet in these children. Further prospective randomized controlled studies are needed, particularly with respect to evaluation of a lactose-restricted diet in children with AP-FGIDs who are lactose malabsorbers. Additionally, the potential role of low-grade gut inflammation in producing symptoms in lactose malabsorbers needs to be investigated in children.
Fructose
Fructose is a monosaccharide of which American children consume a mean of 54.7 g/day (representing approx. 10% of their daily caloric intake) [23]. Fructose is dependent on the glucose transporter 5 (GLUT5) and glucose transporter 2 (GLUT2) for passive absorption.
Fructose Studies in Children with AP-FGIDs
One prospective randomized controlled trial using a fructose-restricted diet has been conducted in children with AP-FGIDs. Wirth et al. [24] randomized 103 children with AP-FGIDs to either a fructose-restricted diet (n = 51) or a no dietary intervention group (n = 52) for 2 weeks. Those on the fructose-restricted diet (irrespective of their fructose hydrogen breath test result) had less pain intensity; however, they did not have a decrease in pain frequency [24]. In a prospective observational study, Wintermeyer et al. [25] placed 75 children with APFGIDs, all of whom had a positive fructose breath test, on a restricted fructose diet. Overall pain frequency and pain severity decreased while on the diet [25].
Three retrospective fructose-related studies have been completed. In 32 children with an AP-FGID, Gomara et al. [9] completed fructose hydrogen breath testing using various doses of fructose, including 1, 15, and 45 g. They found that 11 (34%) of the 32 studied children had fructose malabsorption at either the 15 or 45 g doses. Of these 11, 9 (82%) had a significant improvement on a 2-week dietitian-recommended fructose-restricted diet [9]. Escobar et al. [26] completed fructose breath testing using 1 g/ kg (up to 25 g) in 222 children with AP-FGIDs. Of these, 121 (55%) had fructose malabsorption, of whom 93 (77%) had improvement on a dietitian-recommended low-fructose diet. Dabritz et al. [27] included fructose hydrogen breath testing in their retrospective review and found that 55/142 (39%) children had fructose malabsorption. As several in the Dabritz cohort had multiple positive carbohydrate tests, the number of children who specifically responded to a fructose-restricted diet is unclear.
Sorbitol
No prospective studies regarding sorbitol restriction have been completed in children with AP-FGIDs. Hyams [28] published a case report describing a 15-year-old girl with chronic abdominal pain attributed to sorbitol ingestion from sugar-free gum which improved with elimination of the sorbitol source. In their retrospective study of hydrogen breath testing in children with RAP, Dabritz et al. [27] found that 109/146 (75%) children had sorbitol malabsorption; 27/31 (87%) improved on a sorbitol-restricted diet.
FODMAP Carbohydrates ( table 1 )
FODMAP carbohydrates include fructose and lactose, fructans, galactans, and polyols (such as sorbitol). Fructans are consumed primarily from wheat in the Western diet, with an average consumption ranging from approximately 4.4 to 6.7 g/day in children in the United States [29]. In the Western diet, galactans are consumed primarily from legumes and beans. Polyols are sugar alcohols such as sorbitol and xylitol.
Fructans, galactans, and polyols have unique bonds which are not able to be hydrolyzed by human enzymes. As such, following ingestion, the vast majority of these sugars enter the human colon essentially intact [30]. Within the colon, they may be metabolized by the gut bacteria, which contain enzymes with the ability to metabolize complex carbohydrates [31].
FODMAP Evidence in Childhood AP-FGIDs
Two prospective studies – one an open-label pilot study and the second one a randomized controlled trial – have evaluated a low-FODMAP diet in children with IBS. In the open-label study, 8 children with IBS were instructed by a dietitian to follow a low-FODMAP diet for 1 week [32]. The group as a whole had a decrease in abdominal pain frequency, with 4 children having a ≥ 50% decrease in abdominal pain frequency as compared to baseline [32] . In the randomized double-blind crossover trial, children with IBS (n = 33) received a low- FODMAP or typical American childhood diet for 48 h [33] . The group as a whole had fewer abdominal pain episodes during the low-FODMAP diet. Those who had significant improvement (>50% decrease in abdominal pain frequency) on the low-FODMAP diet, compared to those who did not, had a gut microbiome composition that was enriched in bacteria with high saccharolytic potential (e.g., Faecalibacterium prausnitzii ) [33].
Sucrose and Starch
Sucrose and starch are normally easily hydrolyzed and absorbed in the small intestine through the activity of sucrase- isomaltase (which hydrolyzes both sucrose and starch) and maltase-glucoamylase (which hydrolyzes starch) [34]. The activities of these enzymes may be evaluated using the Dahlqvist method from duodenal biopsy tissue obtained during upper endoscopy [35].
Carbohydrate enzyme deficiencies related to sucrose and starch digestion have been investigated in children with AP-FGIDs. Children with AP-FGID (n = 44) undergoing upper GI endoscopy for the evaluation of abdominal pain, vomiting, or gastroesophageal reflux were evaluated for lactase, sucrase, and glucoamylase activities [36]. Low enzyme activities were found in 32, 34, and 28% of children, respectively, with some children having a combination of enzyme deficiencies [36]. These findings are supported by those of El-Chammas et al. [37] who evaluated disaccharidase activity in 203 children with APFGIDs. Low enzyme levels for lactase, sucrose, glucoamylase, and palatinase (a measure of isomaltase) were found in 37, 21, 25, and 8%, respectively [37]. However, neither study found a correlation between enzyme activity levels and GI symptoms. In addition, the studies did not have a dietary intervention component. Future studies are needed to further investigate the significance of disaccharidase deficiencies and potential dietary or other interventions in children with AP-FGIDs.
Future studies are needed to further investigate the significance of disaccharidase deficiencies and potential dietary or other interventions in children with AP-FGIDs
Fiber Therapy in Childhood AP-FGIDs
Proposed Mechanisms
The rationale for fiber therapy for AP-FGIDs primarily relates to using either soluble fiber or insoluble fiber. Soluble fiber is able to absorb water and maintain the hydration of stool [38]. Insoluble fiber has the potential ability to mechanically stimulate/irritate the gut mucosa and induce a laxative effect through secretion of mucous and water, resulting in more rapid transit through the colon [38] . Fiber that is not easily fermented and is able to maintain its gel-like property, such as psyllium, provides increased water-holding capacity and regulation of stool form [38] . In contrast to soluble fiber, insoluble fiber (e.g., bran) has been shown to potentially exacerbate GI symptoms in adults with IBS [39].
Evidence in Childhood AP-FGIDs
Soluble fiber has demonstrated efficacy in randomized controlled trials in children with AP-FGIDs. In a double-blind randomized controlled trial with 52 children with AP-FGIDs, Feldman et al. [40] compared 10 g of corn fiber (a type of soluble fiber) supplementation for 2 weeks to placebo. With the primary endpoint of a 50% reduction in abdominal pain frequency, 13/26 (50%) of those with fiber supplementation achieved the endpoint compared to 7/26 (27%) of those receiving placebo (p < 0.04) [40].
Soluble fiber has demonstrated efficacy in children with AP-FGIDs
In a double-blind randomized controlled trial with 32 children with RAP who were hospitalized for their abdominal pain, Christensen [41] reported no benefit using 7 weeks of ispaghula husk (psyllium – containing greater soluble than insoluble fiber properties) [38] . However, as this report is in the form of a letter to the editor, important information is missing (e.g., p values, standard deviations), making interpretation of the results difficult [41] . A prospective randomized controlled trial recently published as an abstract suggests that psyllium may be beneficial in children with IBS, though full details are still not published as of the time of this review [42] . Retrospective studies suggest a benefit of increased fiber intake in reducing the risk of abdominal pain in children [43, 44].
Disclosure Statement
B.P.C. has received research support from the National Institutes of Health and QOL Medical, Inc., and was a consultant for Mead Johnson Nutrition. R.J.S. has received research support from the National Institutes of Health and is a consultant for Mead Johnson Nutrition.
Financial and/or intellection support during the completion of this review was provided by NIH K23 DK101688 (B.P.C.) and NIH R01 NR013497 as well as the Daffy’s Foundation (R.J.S.), the USDA/ARS under Cooperative Agreement No. 6250-51000-043 (R.J.S.), and P30 DK56338, which funds the Texas Medical Center Digestive Disease Center (B.P.C., R.J.S.).
The writing of this article was supported by Nestlé Nutrition Institute.
References
Chitkara DK, Rawat DJ, Talley NJ: The epidemiology of childhood recurrent abdominal pain in Western countries: a systematic review. Am J Gastroenterol 2005; 100: 1868– 1875.
Hyams JS, Burke G, Davis PM, Rzepski B, Andrulonis PA: Abdominal pain and irritable bowel syndrome in adolescents: a communitybased study. J Pediatr 1996; 129: 220–226.
Youssef NN, Murphy TG, Langseder AL, Rosh JR: Quality of life for children with functional abdominal pain: a comparison study of patients’ and parents’ perceptions. Pediatrics 2006; 117: 54–59.
Chitkara DK, van Tilburg MA, Blois-Martin N, Whitehead WE: Early life risk factors that contribute to irritable bowel syndrome in adults: a systematic review. Am J Gastroenterol 2008; 103: 765–774.
Rasquin A, DiLorenzo C, Forbes D, Guiraldes E, Hyams JS, Staiano A, Walker LS: Childhood functional gastrointestinal disorders: child/adolescent. Gastroenterology 2006; 130: 1527–1537.
Carlson MJ, Moore CE, Tsai CM, Shulman RJ, Chumpitazi BP: Child and parent perceived food-induced gastrointestinal symptoms and quality of life in children with functional gastrointestinal disorders. J Acad Nutr Diet 2014; 114: 403–413.
Austin GL, Ogden LG, Hill JO: Trends in carbohydrate, fat, and protein intakes and association with energy intake in normalweight, overweight, and obese individuals: 1971–2006. Am J Clin Nutr 2011; 93: 836–843.
Barr RG, Levine MD, Watkins JB: Recurrent abdominal pain of childhood due to lactose intolerance. N Engl J Med 1979; 300: 1449– 1452
Gomara RE, Halata MS, Newman LJ, Bostwick HE, Berezin SH, Cukaj L, et al: Fructose intolerance in children presenting with abdominal pain. J Pediatr Gastroenterol Nutr 2008; 47: 303–308.
Murray K, Wilkinson-Smith V, Hoad C, Costigan C, Cox E, Lam C, et al: Differential effects of FODMAPs (fermentable oligo-, di-, mono-saccharides and polyols) on small and large intestinal contents in healthy subjects shown by MRI. Am J Gastroenterol 2014; 109: 110–119.
Yang J, Deng Y, Chu H, Cong Y, Zhao J, Pohl D, et al: Prevalence and presentation of lactose intolerance and effects on dairy product intake in healthy subjects and patients with irritable bowel syndrome. Clin Gastroenterol Hepatol 2013; 11: 262–268.
Matthews SB, Waud JP, Roberts AG, Campbell AK: Systemic lactose intolerance: a new perspective on an old problem. Postgrad Med J 2005; 81: 167–173.
Fusch G, Choi A, Rochow N, Fusch C: Quantification of lactose content in human and cow’s milk using UPLC-tandem mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci 2011; 879: 3759–3762.
Deng Y, Misselwitz B, Dai N, Fox M: Lactose intolerance in adults: biological mechanism and dietary management. Nutrients 2015; 7: 8020–8035.
Misselwitz B, Pohl D, Fruhauf H, Fried M, Vavricka SR, Fox M: Lactose malabsorption and intolerance: pathogenesis, diagnosis and treatment. United European Gastroenterol J 2013; 1: 151–159.
Hertzler SR, Savaiano DA: Colonic adaptation to daily lactose feeding in lactose maldigesters reduces lactose intolerance. Am J Clin Nutr 1996; 64: 232–236.
Martini MC, Smith DE, Savaiano DA: Lactose digestion from flavored and frozen yogurts, ice milk, and ice cream by lactase-deficient persons. Am J Clin Nutr 1987; 46: 636– 640.
Savaiano DA, Levitt MD: Milk intolerance and microbe-containing dairy foods. J Dairy Sci 1987; 70: 397–406.
Gudmand-Hoyer E, Simony K: Individual sensitivity to lactose in lactose malabsorption. Am J Dig Dis 1977; 22: 177–181.
Lebenthal E, Rossi TM, Nord SK, Branski D: Recurrent abdominal pain and lactose absorption in children. Pediatrics 1981; 67: 828– 832.
Gremse DA, Greer AS, Vacik J, DiPalma JA: Abdominal pain associated with lactose ingestion in children with lactose intolerance. Clin Pediatr (Phila) 2003; 42: 341–345.
Dearlove J, Dearlove B, Pearl K, Primavesi R: Dietary lactose and the child with abdominal pain. Br Med J 1983; 286: 1936–1936.
Vos MB, Kimmons JE, Gillespie C, Welsh J, Blanck HM: Dietary fructose consumption among US children and adults: the Third National Health and Nutrition Examination Survey. Medscape J Med 2008; 10: 160.
Wirth S, Klodt C, Wintermeyer P, Berrang J, Hensel K, Langer T, et al: Positive or negative fructose breath test results do not predict response to fructose restricted diet in children with recurrent abdominal pain: results from a prospective randomized trial. Klin Padiatr 2014; 226: 268–273.
Wintermeyer P, Baur M, Pilic D, Schmidt- Choudhury A, Zilbauer M, Wirth S: Fructose malabsorption in children with recurrent abdominal pain: positive effects of dietary treatment. Klin Padiatr 2012; 224: 17–21.
Escobar MA Jr, Lustig D, Pflugeisen BM, Amoroso PJ, Sherif D, Saeed R, et al: Fructose intolerance/malabsorption and recurrent abdominal pain in children. J Pediatr Gastroenterol Nutr 2014; 58: 498–501.
Dabritz J, Muhlbauer M, Domagk D, Voos N, Hennebohl G, Siemer ML, et al: Significance of hydrogen breath tests in children with suspected carbohydrate malabsorption. BMC Pediatr 2014; 14: 59.
Moshfegh AJ, Friday JE, Goldman JP, Ahuja JK: Presence of inulin and oligofructose in the diets of Americans. J Nutr 1999; 129: 1407S–1411S.
Barrett JS, Gibson PR: Fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) and nonallergic food intolerance: FODMAPs or food chemicals? Therap Adv Gastroenterol 2012; 5: 261– 268.
Flint HJ, Scott KP, Duncan SH, Louis P, Forano E: Microbial degradation of complex carbohydrates in the gut. Gut Microbes 2012; 3: 289–306.
Chumpitazi BP, Hollister EB, Oezguen N, Tsai CM, McMeans AR, Luna RA, et al: Gut microbiota influences low fermentable substrate diet efficacy in children with irritable bowel syndrome. Gut Microbes 2014; 5: 165–75.
Chumpitazi BP, Cope JL, Hollister EB, Tsai CM, McMeans AR, Luna RA, et al: Randomised clinical trial: gut microbiome biomarkers are associated with clinical response to a low FODMAP diet in children with the irritable bowel syndrome. Aliment Pharmacol Ther 2015; 42: 418–427.
Dahlqvist A, Hammond JB, Crane RK, Dunphy JV, Littman A: Assay of disaccharidase activities in peroral biopsies of the small-intestinal mucosa. Acta Gastroenterol Belg 1964; 27: 543–555.
Karnsakul W, Luginbuehl U, Hahn D, Sterchi E, Avery S, Sen P, et al: Disaccharidase activities in dyspeptic children: biochemical and molecular investigations of maltase-glucoamylase activity. J Pediatr Gastroenterol Nutr 2002; 35: 551–556.
El-Chammas K, Williams SE, Miranda A: Disaccharidase deficiencies in children with chronic abdominal pain. JPEN J Parenter Enteral Nutr 2015, Epub ahead of print.
McRorie JW Jr: Evidence-based approach to fiber supplements and clinically meaningful health benefits. Part 2. What to look for and how to recommend an effective fiber therapy. Nutr Today 2015; 50: 90–97.
Hebden JM, Blackshaw E, D’Amato M, Perkins AC, Spiller RC: Abnormalities of GI transit in bloated irritable bowel syndrome: effect of bran on transit and symptoms. Am J Gastroenterol 2002; 97: 2315–2320.
Feldman W, McGrath P, Hodgson C, Ritter H, Shipman RT: The use of dietary fiber in the management of simple, childhood, idiopathic, recurrent abdominal pain. Results in a prospective, double-blind, randomized, controlled trial. Am J Dis Child 1985; 139: 1216–1218.
Christensen MF: Recurrent abdominal pain and dietary fiber. Am J Dis Child 1986; 140: 738–739.
Shulman RJ, Cain K, Czyzewski D, Self M, Weidler E, Devaraj S, et al: Randomized, double blind trial of psyllium fiber in children with irritable bowel syndrome (IBS). Gastroenterology 2015; 148:S120.
Huang RC, Palmer LJ, Forbes DA: Prevalence and pattern of childhood abdominal pain in an Australian general practice. J Paediatr Child Health 2000; 36: 349–353.
Paulo AZ, Amancio OM, de Morais MB, Tabacow KM: Low-dietary fiber intake as a risk factor for recurrent abdominal pain in children. Eur J Clin Nutr 2006; 60: 823–827.
Rodriguez-Fandino O, Hernandez-Ruiz J, Schmulson M: From cytokines to toll-like receptors and beyond – current knowledge and future research needs in irritable bowel syndrome. J Neurogastroenterol Motil 2010; 16: 363–373.
Barrett JSG, Gibson PR: Clinical ramifications of malabsorption of fructose and other short-chain carbohydrates. Pract Gastroenterol 2007; 53: 51–65.
Liebman WM: Recurrent abdominal pain in children: lactose and sucrose intolerance, a prospective study. Pediatrics 1979; 64: 43–45.
Blumenthal I, Kelleher J, Littlewood JM: Recurrent abdominal pain and lactose intolerance in childhood. Br Med J (Clin Res Ed) 1981; 282: 2013–2014.
Wald A, Chandra R, Fisher SE, Gartner JC, Zitelli B: Lactose malabsorption in recurrent abdominal pain of childhood. J Pediatr 1982; 100: 65–68.
Bhan MK, Arora NK, Ghai OP, Dhamija NK, Nayyar S, Fotedar A: Lactose and milk intolerance in recurrent abdominal pain of childhood. Indian J Pediatr 1982; 49: 199–202.
Webster RB, Dipalma JA, Gremse DA: Lactose maldigestion and recurrent abdominal pain in children. Dig Dis Sci 1995; 40: 1506– 1510.
Ceriani R, Zuccato E, Fontana M, Zuin G, Ferrari L, Principi N, Paccagnini S, Mussini E: Lactose malabsorption and recurrent abdominal pain in Italian children. J Pediatr Gastroenterol Nutr 1988; 7: 852–857.
Gremse DA, Nguyenduc GH, Sacks AI, Dipalma JA: Irritable bowel syndrome and lactose maldigestion in recurrent abdominal pain in childhood. South Med J 1999; 92: 778– 781.
Boey CC: Lactase deficiency among Malaysian children with recurrent abdominal pain. J Paediatr Child Health 2001; 37: 157– 160.
Gijsbers CF, Kneepkens CM, Buller HA: Lactose and fructose malabsorption in children with recurrent abdominal pain: results of double-blinded testing. Acta Paediatr 2012; 101:e411–e415.
Ockeloen LE, Deckers-Kocken JM: Shortand long-term effects of a lactose-restricted diet and probiotics in children with chronic abdominal pain: a retrospective study. Complement Ther Clin Pract 2012; 18: 81–84.