Diet and growth of vegetarian and vegan children
The prevalence of plant-based diets, both vegetarian and vegan, are increasing in children and adolescents, when energy and nutrient demands are the highest. While recent studies have shown mostly comparable anthropometrics between omnivore and vegetarian children, as well as in energy-intake. For other measures, such as in micronutrient status, are lower and may require supplementation for the plant-based fed children. Generally, results for the plant-based group were favorable such as in fat mass, blood lipid profile, and for fibre, sugar, folate, magnesium and iron intakes. However, long-term clinical relevance of the results and the plant-based diets’ implications for health remain unclear. It is recommended that professional societies should develop country-specific food-based dietary guidelines adapted to the special dietary habits for children on plant-based diets.
ABSTRACT
The prevalence of plant-based diets, that is, vegetarian (without meat and fish) and vegan (plant foods only) diets, is increasing also among children and adolescents, and energy and nutrient requirements are highest during this age. Hence the question emerges whether and, if so, how much animal-source food should be included in a healthy and sustainable diet. Recent studies, published 2018–2023, mostly showed comparable anthropometrics between omnivore and vegetarian children, however, fat mass was lower in vegetarians or vegans. Results on marker of iron status were inconsistent. Vitamin B12 status was lower without supplementation, but did not differ between groups when supplementation prevalence was high. Blood lipid profile seems to be more favourable in plant-based groups. Bone mineral density was lower in vegetarians and vegans, but differences attenuated after adjustment. Nevertheless, the long-term clinical relevance of these results remains unclear. Energy intake did not differ between groups and was in the recommended range, although protein intake was lower in vegetarians and vegans. Reported calcium intakes did not differ or were lower in vegetarians compared with omnivores, and were lowest in vegans. More favourable intakes in subjects on plant-based diets were found for fibre, sugar, folate, magnesium and iron. All but one study were cross- sectional, and longitudinal studies of both vegetarian and vegan children/adolescents are required to prospectively examine associations of plant-based diets with health.
Professional societies should develop country-specific food-based dietary guidelines adapted to the special dietary habits for children on plant-based diets.
INTRODUCTION
There is currently controversy about whether and, if so, how much animal-source food should be included in a healthy and sustain- able diet.1 2 This issue is particularly relevant for children.3 4 Due to growth and development, energy and nutrient requirements per kg body weight are higher than in later, less vulnerable stages of life and malnutrition can impair growth and development, sometimes irreversibly. The suitability of plant-based diets, especially vegetarian (without meat and fish) and vegan (plant foods only) diets, in this age group, is, therefore, an unsolved issue. Hence, this review aims to describe the current evidence on growth, health and nutrient adequacy of vegetarian and vegan diets during growth.
PREVALENCE AND MOTIVES
There is an increasing prevalence of individuals consuming a vegetarian or vegan diet in high-income countries.25–7 In the general adult population, it is estimated that around 10% follow a vegetarian diet, and around 1%–2% a vegan diet.2 The prevalence among children and adolescents is not clear.2 In Germany, results from the 2015–2017 EsKiMo II study showed a total of 3.4% vegetarians (1.5% among 6–11-year-olds; 5.1% among 12–17-year-olds). This is a clear increase over the first EsKiMo I study conducted in 2006 (1.6% vegetarians among the 12–17-year-olds; no data available for younger children). Vegetarian diets were more prevalent among girls and in children from families with high economic status.8 These sociodemographic characteristics are consistent with data from studies of adults.7 9
Among adults, animal rights/welfare and ethics is one main motive to follow a plant- based diet, but also health and concerns for environmental sustainability.10 This is in accordance with a German cross-sectional study, in which children and adolescents were asked for their primary motive to consume a vegetarian or vegan diet. The vast majority reported ethical, that is, animal rights motives (ie, rejection of mass farming, right to life for animals or an emotional attachment to animals) as the most important motive for choosing their diet (vegetarians: 70%, vegans: 69%). Environmental reasons (eg, climate protection, resource conservation) were the primary motive for only 7% of vegetarians and 5% of vegans, whereas health played a role as the primary motive for 11% of vegans (vegetarians: 2%). At least 14% of vegetarians and 13% of vegans stated that the motive for their diet was ‘because the parents eat this way’. Those participants indicating the parental diet as the primary motive were significantly younger (8.2±2.2 years), whereas those indicating ethics as the primary motive were slightly older (12.9±3.7 years) than those indicating other motives.11
POSITIONS OF PROFESSIONAL HEALTH ASSOCIATIONS
In some countries, vegetarian and especially vegan child nutrition is seen rather critically. In Germany and Switzerland, a carefully planned vegetarian diet is considered feasible even at growing age, but a vegan diet is not recommended.12 13 The German Society for Paediatric and Adolescent Medicine recommended a balanced, omni- vore diet with a moderate consumption of meat, fish and dairy because nutrient requirements are most easily and most likely met.9 Other professional societies conclude that an appropriately planned (or balanced) vegetarian, including vegan, diet is (or can be) healthy and nutrition- ally adequate in childhood and adolescence, for example, the Academy of Nutrition and Dietetics,7 the Italian Society of Human Nutrition14 or the Canadian Paediatric Society.15 However, these professional societies also list potentially critical nutrients and provide detailed guidance on how to ensure that intakes meet requirements.
POTENTIAL CRITICAL NUTRIENTS
Restrictive diets, excluding animal source foods, have an increased risk of inadequate nutrient intakes, not only because a lower dietary diversity generally decreases the likelihood of adequate nutrient supply. Animal source foods are good sources of some nutrients, for example, for high-quality protein (meat, fish, dairy), riboflavin and calcium (dairy), iodine (fish, dairy), long-chain n-3 fatty acids (fatty fish), selenium (animal-source food) and bioactive compounds including creatine or taurin.1 16 In particular, animal-source foods are the only natural source of vitamin B12.6 9 The bioavailability of some nutrients is also higher from animal-source foods. First, because nutrients are in a readily absorbable form, such as haem iron in meat.1 2 6 Furthermore, some plant foods contain anti-nutritive substances that impair absorption, such as phytates that inhibit the absorption of iron and zinc.1 2 9 However, animal-source foods are also major sources of saturated fatty acids and cholesterol, contribute little to the supply of potassium, magnesium and folate, and lack many health-promoting ingredients such as dietary fibre and phytonutrients (secondary plant compounds).1 2 17
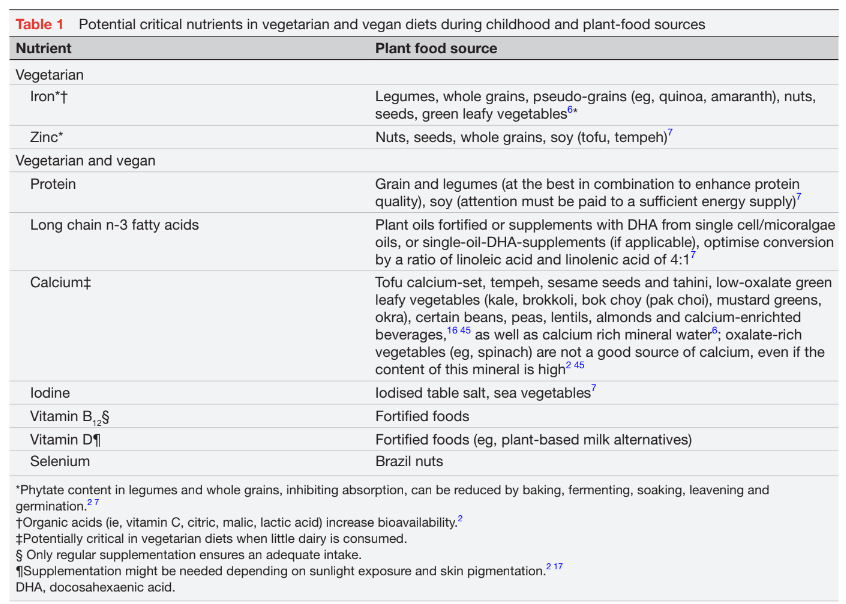
With a vegetarian diet, special attention should there- fore be paid to a sufficient supply of iron and zinc, with a vegan diet additionally to protein, long-chain n-3 fatty acids, calcium, iodine, selenium and in particular vitamin B12 (table 1).
ACTUAL STUDIES ON VEGETARIAN AND VEGAN CHILD NUTRITION
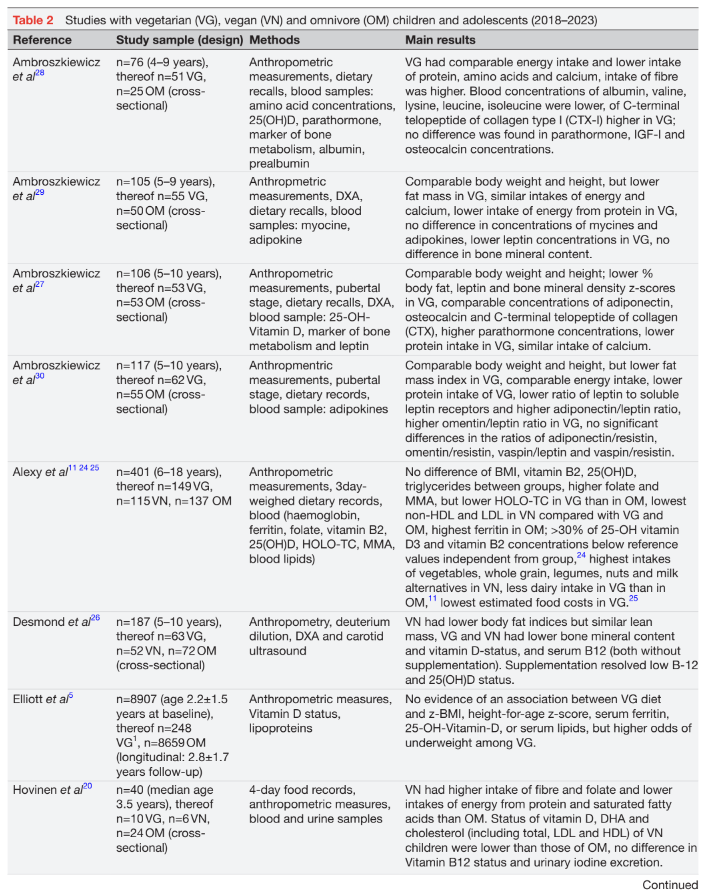
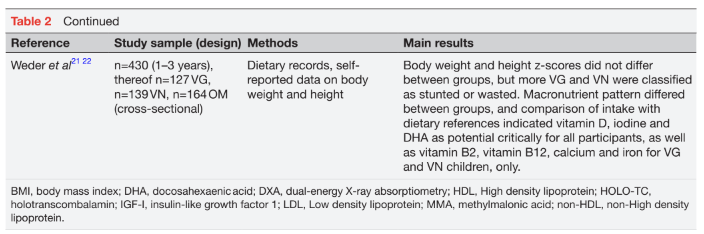
In their 2017 review on vegetarian and vegan diets during childhood, Schürmann et al listed 24 publications from 16 studies published from 1988 to 2013.18 Only two studies were found examining vegan-fed children separately. With the exception of studies in the Adventist setting, which may have some sampling bias, the samples were small and most studies were cross-sectional. Outcomes were heterogeneous. Overall, the growth and body weight of children on plant-based diets were found within the lower reference range. Studies indicated lower or similar biomarkers of iron status in vegetarians compared with omnivore groups.18 However, since these studies were conducted, substantial changes in the food market occurred: the range of foods offered has increased, including with respect to plant-based meat and dairy alternatives.7 19 More dietary supplements are available on the market, and the world wide web has developed into an important source of information about noteworthy aspects of a plant-based diet. However, only a few studies on modern vegetarian and vegan child nutrition have been published so far (table 2).
There was only one longitudinal study (follow-up: 3 years) with a sample of young children (6 months to 8 years) in Canada, conducted between 2008 and 2019.5 The type of diet was self-reported by parents. Of 8907 children, 248 (2.7%) were categorised as vegetarian, of whom 25 were vegan (0.3% of the total sample). The small number of vegan children precluded a separate analysis. Although vegetarian participants were more likely to have Asian ethnicity, mean body mass index (BMI)-z- score and BMI-z-score growth rates did not differ between diet groups. Nevertheless, vegetarian-fed children were slightly less tall than the control group. However, the effect size was small and was estimated to be 0.3 cm for a 3-year-old child. Serum ferritin, 25(OH) vitamin D and serum lipids did not differ between groups. The authors concluded that there were no meaningful differences in growth or the biochemical measures assessed in this study between vegetarian or omnivore children.5
In a small Finnish study, 40 young children from daycare centres, including 24 omnivore, 10 vegetarian and 6 vegan participants, were examined cross-sectionally in 2017.20 No differences in anthropometric measurements (z-scores of heights, BMI and mid-upper arm circumference) were found between groups, although protein intake (% of energy intake), calculated from 4-day estimated dietary records, was lower among vegans. In contrast, fibre and folate intakes were higher in vegans than in omnivores. Blood lipids were lower in the vegan group, vitamin A status was insufficient, but erythrocyte folate was higher. The serum concentration of vitamin B12 was adequate, and no group difference of urinary iodine concentration was found. Furthermore, untargeted metabolomics analysis showed lower concentrations of essential amino acids and docosahexaenoic acid (DHA). The authors conclude that given the observed metabolic differences, the health consequences of a vegan diet in childhood need to be clarified.20
Two studies on vegan and vegetarian diets in Germany were conducted by a working group to which the author of this article belongs: The VeChi-Diet study examined between 2016 and 2018 the diet of 430 children (127 vegetarian, 139 vegan, 164 omnivorous) aged 1–3 years using dietary records.21–23 Although mean z-scores of parental-reported body weight and height did not differ between diet groups, a slightly higher percentage of vegan (3.6%) compared with vegetarian (2.4%) and omnivore (0%) were classified as stunted, and 3.6% of vegan, 0.6% of omnivore and no vegetarian child were classified as wasted.22 Neither energy intake nor energy density differed between diet groups. Protein intake was lowest among vegans and highest among omnivores, but all groups exceeded the dietary reference value of 1g/kg body weight per day by 2.3–2.5-fold. Added sugar was the lowest and fibre intake was highest among vegans.22 Micronutrient intakes showed a significant difference between groups.21 Vegan children had the highest intakes of folate, magnesium and iron, followed by vegetarians. Including dietary supplements, the intake of vitamin B12 was the highest too.21 In a separate evaluation, selenium intake was estimated using a food composition database provided by the European Food Safety Authority. Although vegetarian and vegan children consumed less selenium than omnivorous children, on average, all three groups met the harmonised average requirement for selenium of 17µg/ day.23
Nevertheless, these results were only based on self- reported dietary intake, which is prone to bias social desirability and inaccuracies of food composition data- base. Hence, the VeChi-Youth-Study (conducted 2017– 2019) also examined biomarkers of potential critical nutrients and blood lipids in a sample of 401 German children and adolescents aged 6–18 years.11 24 25 In this study, the SD score of BMI did not differ between vegetarian, vegan and omnivore participants.24 Vegans had no higher rates of iron deficiency anaemia, but ferritin levels were slightly lower,24 which might be beneficial for long-term health.2 Vegans had the lowest non- high-density lipoprotein (non-HDL) and low-density lipoprotein (LDL) concentrations in comparison to vegetarians and omnivores. A high prevalence (>30%) of 25-OH vitamin D3 and vitamin B2 concentrations below reference values were found irrespective of the diet group.24 The food intake pattern of vegan children and adolescents was characterised by higher intakes of whole grains, legumes, nuts and plant-based milk alternatives than those of vegetarians. However, vegetarians in this study also consumed significantly less dairy than the omnivore control group.11 As the affordability of such a plant-based food pattern is repeatedly debated, a further evaluation estimated the food costs of the three diet groups using retail food prices.25 It could be shown that the vegetarian food pattern was the least expensive compared with the omnivore and vegan diet pattern and food costs did not differ significantly between omnivores and vegans.25
In Poland, Desmond et al26 cross-sectionally examined children aged 5–10 years (63 vegetarians, 52 vegans, 72 omnivores) using anthropometry, deuterium dilution, DXA, carotid ultrasound, fasting blood samples, dietary intake and accelerometery data. Vegetarians (−2 cm) and vegans (−3 cm) were shorter than omnivores, but the difference for vegetarians was not significant. However, height z-scores were >0 in all groups, indicating sufficient overall longitudinal growth. Also bone mineral content was lower in both plant-based groups than in omnivores, but the cardiovascular risk profile was healthier in vegans. Furthermore, vegans had lower serum vitamin B12 and 25(OH) vitamin D concentrations, but this difference was not evident in those subgroups using supplements. With respect to iron status, vegans, but not vegetarians had lower haemoglobin and ferritin levels than omnivores.26
Another Polish working group repeatedly recruited vegetarian and omnivore children attending a mother and child health facility and examined several aspects of metabolic health.27–30 The most recent paper described amino acid levels and bone markers in n=51 vegetarian (of whom 9% were vegans) and n=25 omnivorous children aged 4–9 years. Apart from the bone resorption marker CTX-I (C-terminal telopeptide of collagen type I, lower levels among vegetarians), bone markers (para- thormone, Insulin-like growth factor 1, osteocalcin and osteoprotegerin) did not differ significantly between the groups. Protein intake (12.8% of energy intake) was lower but adequate among vegetarians, and blood concentrations of some amino acids (ie, valine, lysine, leucine and isoleucine) were lower too.28
An additional study of 53 vegetarian and 53 omnivore pre-pubertal children examined the aforementioned bone markers and additionally bone mineral density in the lumbar spine by dual-energy X-ray absorptiometry (DXA). Vegetarian children had a lower percentage of fat mass and leptin concentrations. Total and lumbar spine bone mineral density z-scores were lower, and parathormone concentrations were higher than omnivores. Notably, bone mineral density z-scores were positively associated with anthropometric parameters.27
In another Polish sample of pre-pubertal children (53 vegetarian and 50 omnivore children, 5–10 years), there were no significant differences between adipokines (adiponectin, visfatin and omentin).27 Also, serum levels of myokines (myostatin, irisin) did not differ between 55 vegetarian and 50 omnivore children aged 5–9 years. The observed lower leptin levels among vegetarians reflected the lower percentage of body fat.29 Considering all this, studies showed comparable anthropometrics between omnivore and vegetarian children.5 20 24 27 29 30 In one study, height was lower among vegans,26 whereas others found no difference between groups.5 20 22 24 27 29 30 However, especially in the youngest sample, higher prevalence of wasting and stunting than in omnivore children was observed in vegetarian and vegan children22 but the prevalence was nonetheless low, and the longitudinal study found higher odds of being under-weight in vegetarians.5 Fat mass was lower in vegetarians27 29 30 or vegans,26 but not in all studies.30 Accordingly, observed leptin concentrations were lower in vegetarians.27 29 Haemoglobin levels were comparable24 or lower in vegans,26 whereas ferritin was lower in vegetarians24 and vegans24 26 or did not differ.5 Also, results of vitamin D status (lower in vegans20 and without supplementation,26 no difference between groups5 24 27 28 or with supplementation26) and vitamin B12 status (lower without supplementation,26 no difference between groups20 24 26 or with supplementation26) were inconsistent. Blood lipid profile seems to be more favourable in plant-based groups,20 24 26 but this was not observed in all studies.5 Mean values of total bone mineral density z-score were significantly lower in vegetarian than in omnivore children,27 but the authors did not adjust for differences in anthropometrics. In another study, bone mineral content was lower in vegetarians and vegans,26 after adjustment for body height and weight z scores, as well as bone area, these differences attenuated to the null in vegetarians and to –3.7% in vegans.26 Osteocalcin concentrations did not differ between groups,27 28 and results on parathormone were inconsistent.27 28 However, the long-term clinical relevance of these results remains unclear. Energy intake did not differ between groups22 24 26 29 and was in the recommended range,27 30 but protein intake was lower in vegetarians24 26 27 29 30 and vegans.20 24 26 More favourable intakes in subjects on plant-based diets were found for fibre, sugar, folate, magnesium and iron.20 21 26 Reported calcium intakes did not differ27 29 or were lower28 in vegetarians compared with omnivores, and were lowest in vegans.24 26
It must be mentioned that none of these studies was representative of the population at large. This could bias the results, as families who participate voluntarily in scientific studies may have better health awareness than the overall population. However, due to the low prevalence of vegetarian and in particular vegan diets, conducting a representative study would be not feasible and too expensive. Furthermore, only randomised trials could detect the causal effects of plant-based diets on nutrient adequacy and health, but such studies are not possible in children for ethical and compliance reasons. It would be desirable to have more data from prospective, longitudinal studies, as currently, only one longitudinal study with vegetarian-fed children is available. In addition, not all studies presented here distinguished between vegetarian and vegan diets. For the development of science-based food-based dietary guidelines (FBDGs), the development of public health measures for vegetarian and vegan families, and to elucidate divergent results of nutritional status between studies, the description of food intake patterns and supplementation habits would be useful. Studies on vegetarian or vegan diets during weaning are lacking up to now.
DIETARY SUPPLEMENTS
Although dietary supplements, in particular vitamin B12, are recommended in a vegetarian and specifically vegan diet both among adults and children, data on the prevalence of use within plant-based diets are scarce. Sutter and Bender stated that a third to a half of all vegans use supplements,17 and awareness about vitamin B12 is assumed to have strongly increased over the last decades.6 Nevertheless, only very few studies with paediatric samples reported exact data on supplementation practices, even when nutrient status was the main aim.31 In some studies, the use of supplements was even an exclusion criterion in recruitment.18 In one recent Polish study26 (table 2), analyses of vitamin D and vitamin B12 status were presented among vegetarian and vegan children stratified by the use of supplements. Accordingly, 44% of vegans and 34% of vegetarians supplemented vitamin B12, and 32% of vegetarians and 33% of vegans supplemented vitamin D.26 In German studies, the supplementation rate in particular of vitamin B12 was substantially higher: In the German Vechi Youth study, the vast majority of participants supplemented vitamin B12 (vegans: 88%, vegetarians: 52%), and a substantial part of the sample also vitamin D (vegans: 54%, vegetarians: 27%).24 In the Vechi Diet study with a younger sample, 97% of vegans and 35% of vegetarians, reported the use of vitamin B12 supplements.21 In Finland, 83% of vegans and 40% of vegetarians reported the intake of vitamin B12 supplements (vitamin D: 90% of vegetarians and 100% of vegans).20 The reasons for the different study results are unclear. It is possible that families in different countries have different levels of information about the need for supple- mentation, or this is the result of selection bias.
However, there is a lack of scientific knowledge about the optimal dosage of vitamin B12-supplements in a vegetarian or vegan diet due to the high variability of absorption attributable to the frequency of intakes.32 The Italian Society of Human Nutrition suggests vitamin B12 either one daily single dose of 5 µg (6 months to 3 years), 25 µg (4–10 years) and 50 µg from 11 years onwards. Alternatively, daily multi-doses of 2×1 µg (<4 years), 2×2 µg (4–10 years) and 3×2 µg (>11 years) are suggested.14 The Canadian Paediatric Society suggests 5 µg to 10 µg of a daily supplement for infants, children and adolescents,15 whereas the German Society for Paediatric and Adolescent Medicine recommended 5–25 µg/day, depending on a person’s vitamin B12 status and age.9 Although there is no upper limit on vitamin B12-intake and excessive vitamin B12 intake is generally considered safe,6 a maximum limit in dietary vitamin B12-supplements of 25 µg was proposed for adults.33 An alternative supple- mentation strategy, the use of vitamin B12-fortified tooth- paste, has been validated in adults,34 but not in children.
PLANT-BASED DIETS AND LONG-TERM HEALTH
Studies on the long-term health of vegetarian and vegan-fed children are lacking because of the long latent period of non-communicable disease. However, it is well accepted that atherosclerosis starts in childhood.35 Compared with omnivore diets, plant-based diets have been associated with substantial reductions in modifiable risk factors in adults, including atherogenic lipoprotein concentrations, blood glucose, inflammation and blood pressure.2 The obesity risk is also reduced,2 with differences in BMI at least partially attributable to an overall healthier lifestyle.16 This evidence among adults is consistent with the results of some of the studies listed in table 2, which reported lower fat mass percentages26 27 29 and more favourable blood lipids20 24 26 among vegetarian and vegan than in omnivore children.
However, one potential long-term risk with a plant-based diet is bone health. In a recent review, a meta-analysis of 20 studies including 37 134 participants indicated that vegetarians and vegans had lower bone mineral density at the femoral neck and lumbar spine compared with omnivores. Furthermore, vegans had higher fracture rates, indicating clinical relevance.36 Although at least in part the results might be attributable to differences in anthropometric variables,37 38 particular attention should be paid to nutrients that are relevant for bone health and potentially critical in vegetarian and vegan diets, such as protein, calcium and vitamin D.39 This is especially important for children and adolescents, as bone mass accumulation reaches its maximum during early adolescence (9–14 years among girls and 11–16 years among boys) and a high peak bone mass is protective against later osteoporosis and fractures.39
In adults, fracture incidence was reduced regardless of a dietary pattern when calcium intake was at least equal to the estimated average requirement of 525 mg/day.40 Adequacy of vitamin D status supports the absorption of calcium. Whether vegetarian or vegan children should routinely take a vitamin D supplement is not yet answered conclusively.2 17 In the Adventist Health Study 2, a combi- nation of both calcium and vitamin D supplementation, the elevated risk for bone fractures among vegans disappeared.41 Nevertheless, bone health is affected by more than these two nutrients, for example, protein intake and dietary acid load. Repeated bone density measurements in children and adolescents who have been consuming a plant-based diet for a longer period would be desirable.
FOOD-BASED DIETARY GUIDELINES
Not every plant-based food pattern is healthy42 and provides sufficient energy and the full spectrum of nutrients. Deficiencies can occur when vegetarian or vegan diets are not well planned, specifically in the paediatric population. Hence, food based dietary guidelines (FBDG) are necessary to inform families about the selection and combination of plant foods and dietary supplements, if necessary, in particular as motivations to follow a plant-based pattern are not necessarily health-based. Nevertheless, only few plant-based dietary guidelines for children and adolescents exist up to now.43
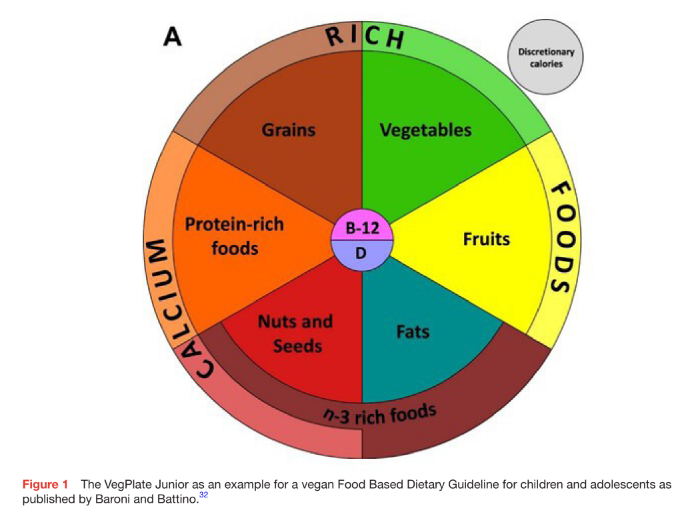
The VegPlate Junior (figure 1)32 provides recommendations for six plant food groups (ie, grains, vegetables, fruits, fats, nuts and seeds and protein-rich foods). On a second level, emphasis was laid on n-3-rich-foods and calcium-rich foods. Supplementation of vitamin B12 and vitamin D is mentioned, too. The VegPlate Junior is based on a selection of the most representative plant foods from the Mediterranean tradition. Dairy and eggs are considered optional. This FBDG was designed to fulfil the Italian and US Dietary Reference Intakes and hence meet all the criteria defining a vegetarian or vegan diet as well-planned.32
The Canadian governmental health recommendations take a different approach and issue one guideline from the age of 2 years44 which can result both in omnivore, vegetarian, or vegan dietary patterns. The Canadian food guidance plate comprises only three segments: vegetables and fruits (half of the plate), whole grain foods and protein foods (a quarter of the plate each). In the protein food group, legumes (beans, peas and lentils), nuts and seeds, as well as fortified soy beverages, tofu and other soy products, are equal to animal-source foods (eggs, lean meat, fish, dairy).44
CONCLUSION
To stop or at least mitigate climate change, a transformation of the diet in Western countries is necessary. Above all, the consumption of meat must be reduced. Further studies are necessary to accompany this transformation and to investigate the long-term effects on nutritional status and health, especially in children. The current studies show that a vegetarian, but also a vegan diet, can ensure sufficient growth. However, especially in young children, height and weight should be monitored regularly to ensure that growth retardation is immediately diagnosed. On the other hand, a vegetarian and vegan diet might be a protective factor against overweight and obesity, not only among adults but also among children.17 Some experts also call for medical supervision of physiologic parameters.2 15 For this purpose, paediatricians should be provided with recommendations regarding the nutrients to be examined, including the appropriate biomarkers, as well as age-specific examination intervals. The limited data on the use of dietary supplements show large differences between countries. The goal must be that all children on vegan diets receive vitamin B12 supplements regularly, and vegetarian-fed children at least occasionally.
A vegetarian but especially a vegan diet for children should be well planned. However, it is important to acknowledge that even poorly planned omnivore diets, for example, a ‘Western Style’ dietary pattern comprising large amounts of animal-source foods, refined grains, salt and sugar, are not without risk16 as the high prevalence of overweight and obesity already during the growing age show. By a combination of a wide range of plant foods and the use of supplements, energy and nutrient intake in children’s diets can also be achieved by partially or even completely avoiding animal foods. Just as with omnivore diets, families need evidence-based and practical information on how a vegetarian and/or vegan diet should be composed for their children. For this, further education in the context of evidence-based FBDG is necessary. For this purpose, professional societies should develop country-specific FBDGs adapted to the respective dietary habits and the regional food market for children on plant-based diets.
___________________________________________
Contributors. UA wrote the paper.
Funding. The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests. None declared.
Patient consent for publication Not applicable.
Ethics approval Not applicable.
Provenance and peer review Not commissioned; externally peer reviewed. Special Issue—Annales Nestle—Foods for the Future and their Potential Impact on Child Nutrition by Meyer, Rosan, Imperial College London, United Kingdom of Great Britain and Northern Ireland by Prentice, Andrew, MRC Unit The Gambia at LSHTM, Gambia.
REFERENCES
1 Beal T, Gardner CD, Herrero M, et al. Friend or foe? The role of animal-source foods in healthy and environmentally sustainable diets. J Nutr 2023;153:409–25.
2 Craig WJ, Mangels AR, Fresán U, et al. The safe and effective use of plant-based diets with guidelines for health professionals. Nutrients 2021;13:4144.
3 Leroy F, Barnard ND. Children and adults should avoid consuming animal products to reduce risk for chronic disease: NO. Am J Clin Nutr 2020;112:931–6.
4 Barnard ND, Leroy F. Children and adults should avoid consuming animal products to reduce risk for chronic disease: YES. Am J Clin Nutr 2020;112:937–40.
5 Elliott LJ, Keown-Stoneman CDG, Birken CS, et al. Vegetarian diet, growth, and nutrition in early childhood: a longitudinal cohort study. Pediatrics 2022;149:e2021052598.
6 Koeder C, Perez-Cueto FJA. Vegan nutrition: a preliminary guide for health professionals. Crit Rev Food Sci Nutr 2022;2022:1–38.
7 Melina V, Craig W, Levin S. Position of the academy of nutrition and dietetics: vegetarian diets. J Acad Nutr Diet 2016;116:1970–80.
8 Patelakis E, Lage Barbosa C, Haftenberger M, et al. Prevalence of vegetarian diet among children and adolescents in Germany: results from Eskimo II. Ernahrungs Umschau 2019;66:85–91.
9 Rudloff S, Bührer C, Jochum F, et al. Vegetarian diets in childhood and adolescence position paper of the Nutrition Committee, German Society for Paediatric and Adolescent Medicine (DGKJ). Mol Cell Pediatr 2019;6:4.
10 Janssen M, Busch C, Rödiger M, et al. Motives of consumers following a vegan diet and their attitudes towards animal agriculture. Appetite 2016;105:643–51.
11 Alexy U, Fischer M, Weder S, et al. Food group intake of children and adolescents (6-18 years) on a vegetarian, vegan or omnivore diet: results of the VeChi youth study. Br J Nutr 2022;128:851–62.
12 Richter M, Boeing H, Grünewald-Funk D, et al. Vegan diet: position of the German nutrition society (DGE). Ernahrungs Umschau 2016;63:92–102.
13 Federal Commission for Nutrition (FCN) (Schweizerische Eidgenossenschaft). Vegan diets: review of nutritional benefits and risks: expert report of the FCN. 2018. Available: www.blv.admin. ch/blv/en/home/das-blv/organisation/kommissionen/eek/vor-und- nachteile-vegane-ernaehrung.html
14 Agnoli C, Baroni L, Bertini I, et al. Position paper on vegetarian diets from the working group of the Italian society of human nutrition. Nutr Metab Cardiovasc Dis 2017;27:1037–52.
15 Amit M. Vegetarian diets in children and adolescents. Paediatr Child Health 2010;15:303–14.
16 Moreno LA, Meyer R, Donovan SM, et al. Perspective: striking a balance between planetary and human health: is there a path forward Advances in Nutrition 2022;13:355–75.
17 Sutter DO, Bender N. Nutrient status and growth in vegan children.
Nutr Res 2021;91:13–25.
18 Schürmann S, Kersting M, Alexy U. Vegetarian diets in children: a systematic review. Eur J Nutr 2017;56:1797–817.
19 Scholz-Ahrens KE, Ahrens F, Barth CA. Nutritional and health attributes of milk and milk imitations. Eur J Nutr 2020;59:19–34.
20 Hovinen T, Korkalo L, Freese R, et al. Vegan diet in young children remodels metabolism and challenges the statuses of essential nutrients. EMBO Mol Med 2021;13:e13492.
21 Weder S, Keller M, Fischer M, et al. Intake of micronutrients and fatty acids of vegetarian, vegan, and omnivorous children (1-3 years) in Germany (Vechi diet study). Eur J Nutr 2022;61:1507–20.
22 Weder S, Hoffmann M, Becker K, et al. Energy, Macronutrient intake, and Anthropometrics of vegetarian, Vegan, and omnivorous children (1-3 years) in Germany (Vechi diet study). Nutrients 2019;11:832.
23 Weder S, Zerback EH, Wagener SM, et al. How does selenium intake differ among children (1-3 years) on vegetarian, vegan, and omnivorous diets? Results of the Vechi diet study. Nutrients 2022;15:34.
24 Alexy U, Fischer M, Weder S, et al. Nutrient intake and status of German children and adolescents consuming vegetarian, vegan or omnivore diets: results of the VeChi youth study. Nutrients 2021;13:1707.
25 Hohoff E, Zahn H, Weder S, et al. Food costs of children and adolescents consuming vegetarian, vegan or omnivore diets: results of the cross-sectional VeChi youth study. Nutrients 2022;14:4010.
26 Desmond MA, Sobiecki JG, Jaworski M, et al. Growth, body composition, and cardiovascular and nutritional risk of 5- to 10-Y-old children consuming vegetarian, vegan, or omnivore diets. Am J Clin Nutr 2021;113:1565–77.
27 Ambroszkiewicz J, Chełchowska M, Szamotulska K, et al. Bone status and adipokine levels in children on vegetarian and omnivorous diets. Clin Nutr 2019;38:730–7.
28 Ambroszkiewicz J, Gajewska J, Mazur J, et al. Dietary intake and circulating amino acid concentrations in relation with bone
metabolism markers in children following vegetarian and omnivorous diets. Nutrients 2023;15:1376.
29 Ambroszkiewicz J, Gajewska J, Mazur J, et al. Does a vegetarian diet affect the levels of myokine and adipokine in prepubertal children? J Clin Med 2021;10:3995.
30 Ambroszkiewicz J, Chełchowska M, Rowicka G, et al. Anti- inflammatory and pro-inflammatory adipokine profiles in children on vegetarian and omnivorous diets. Nutrients 2018;10:1241.
31 Ambroszkiewicz J, Klemarczyk W, Chełchowska M, et al. Serum homocysteine, folate, vitamin B12 and total antioxidant status in vegetarian children. Adv Med Sci 2006;51:265–8.
32 Baroni L, Goggi S, Battino M. Planning well-balanced vegetarian diets in infants, children, and adolescents: the vegplate Junior. J Acad Nutr Diet 2019;119:1067–74.
33 Weißenborn A, Bakhiya N, Demuth I, et al. Höchstmengen Für Vitamine und Mineralstoffe in Nahrungsergänzungsmitteln. J Consum Prot Food Saf 2018;13:25–39.
34 Siebert A-K, Obeid R, Weder S, et al. Vitamin B-12-fortified toothpaste improves vitamin status in Vegans: a 12-wk randomized placebo-controlled study. Am J Clin Nutr 2017;105:618–25.
35 Desmond MA, Sobiecki J, Fewtrell M, et al. Plant-based diets for children as a means of improving adult cardiometabolic health. Nutr Rev 2018;76:260–73.
36 Iguacel I, Miguel-Berges ML, Gómez-Bruton A, et al. Veganism, vegetarianism, bone mineral density, and fracture risk: a systematic review and meta-analysis. Nutr Rev 2019;77:452–3.
37 Tong TYN, Appleby PN, Armstrong MEG, et al. Vegetarian and vegan diets and risks of total and site-specific fractures: results from the prospective EPIC-Oxford study. BMC Med 2020;18:353.
38 Karavasiloglou N, Selinger E, Gojda J, et al. Differences in bone mineral density between adult vegetarians and nonvegetarians become marginal when accounting for differences in anthropometric factors. J Nutr 2020;150:1266–71.
39 Abrams SA. Bone health in school age children: effects of nutritional intake on outcomes. Front Nutr 2021;8:773425.
40 Appleby P, Roddam A, Allen N, et al. Comparative fracture risk in vegetarians and nonvegetarians in EPIC-Oxford. Eur J Clin Nutr 2007;61:1400–6.
41 Thorpe DL, Beeson WL, Knutsen R, et al. Dietary patterns and hip fracture in the adventist health study 2: combined vitamin D and calcium supplementation mitigate increased hip fracture risk among vegans. Am J Clin Nutr 2021;114:488–95.
42 Kim H, Caulfield LE, Rebholz CM. Healthy plant-based diets are associated with lower risk of all-cause mortality in US adults. J Nutr 2018;148:624–31.
43 Klapp A-L, Feil N, Risius A. A global analysis of national dietary guidelines on plant-based diets and substitutions for animal-based foods. Curr Dev Nutr 2022;6:nzac144.
44 Government of Canada. Canada’s food guide: eat a variety of healthy foods each day. 2023. Available: https://food-guide.canada.ca/en/
45 Wright NS, Smith M. Guidelines suggesting children avoid plant-based milks: a closer examination. Matern Child Health J 2020;24:1189–92.