Long-Chain Polyunsaturated Fatty Acids and Clinical Outcomes of Preterm Infants
45 min read
Key insights
Infants who are born prematurely have unique nutritional requirements due to their immaturity. The standard nutritional management of premature infants results in deficiencies in long-chain polyunsaturated fatty acids (LCPUFAs), particularly docosahexaenoic acid (DHA). Providing higher levels of DHA than routinely given is associated with better neurological and clinical outcomes.
Current knowledge
Infants who are born premature or extremely premature have a high risk of morbidities and mortality. During their initial hospitalization, parenteral nutrition is given to meet their nutritional needs. LCPUFAs play important roles in perinatal growth and development and are therefore an important component of nutrition for these infants. In premature infants, the endogenous capacity for synthesizing DHA and eicosapentaenoic acid is not sufficient to meet their requirements for these critical LCPUFAs. Limited supply of LCPUFAs through external nutritional sources further exacerbates the problem.
Practical implications
Currently, the nutritional management of preterm infants results in an early and severe deficit in DHA. The smallest and most premature infants are especially vulnerable; these infants are the most likely to benefit from high-dose DHA supplementation. Due to their immaturity, premature infants are at risk of concomitant diseases such as bronchopulmonary dysplasia, retinopathy of prematurity, necrotizing enterocolitis, and white matter injury of the brain. Supplementation with LCPUFAs including DHA has been used to alleviate these risks, possibly as a consequence of their anti-inflammatory effects. Despite some conflicting findings, the main message from clinical studies indicates that supplementing with adequate levels of LCPUFAs is an important step towards optimizing the clinical outcomes of premature infants.
Recommended reading
Zhang P, Lavoie PM, Lacaze-Masmonteil T, Rhainds M, Marc I: Omega-3 long-chain polyunsaturated fatty acids for extremely preterm infants: a systematic review. Pediatrics 2014;134:120–134.
Recent clinical trials show that providing larger amounts of docosahexaenoic acid (DHA) than currently and routinely provided is associated with better neurological outcomes at 18 months to 2 years.
There is growing evidence that omega-3 long-chain polyunsaturated fatty acids, particularly DHA, may reduce the incidence or severity of neonatal morbidities by affecting different steps of the immune and anti-inflammatory response.
Long-chain polyunsaturated fatty acids (LCPUFAs) play specific roles during the perinatal period and are very important nutrients to consider. The possible effects of LCPUFAs, particularly docosahexaenoic acid (DHA), on various clinical outcomes of preterm infants are discussed in this paper. Since DHA accumulates in the central nervous system during development, a lot of attention has focused on the effects of DHA on neurodevelopment. Experimental studies as well as recent clinical trials show that providing larger amounts of DHA than currently and routinely provided is associated with better neurological outcomes at 18 months to 2 years. This early advantage, however, does not seem to translate into detectable change in visual and neurodevelopmental outcomes or behavior when assessed in childhood. There is growing evidence that, in addition to effects on development, omega-3 LCPUFAs may reduce the incidence or severity of neonatal morbidities by affecting different steps of the immune and anti-inflammatory response. Studies in preterm infants suggest that the omega-3 LCPUFAs may play a significant role by reducing the risk of bronchopulmonary dysplasia, necrotizing enterocolitis and possibly retinopathy of prematurity and sepsis. Overall, evidence is increasing to support the benefits of high-dose DHA for various health outcomes of preterm infants. These findings are of major clinical relevance mainly because infants born preterm are at particularly high risk for a nutritional deficit in omega-3 fatty acids, predisposing to adverse neonatal outcomes. Further studies are warranted to address these issues as well as to more precisely determine the LCPUFA requirement in order to favor the best possible outcomes of preterm infants.
Introduction
Preterm birth is the leading cause of child mortality in high- and middle-income countries. The risk of morbidity and mortality in infants born very and extremely premature has been well documented [1]. Fortunately, improved pre- and postnatal care has led to reduced mortality and morbidity. However, the risk of severe medical disabilities increases sharply with decreasing gestational age (GA) at birth [1].
During the initial part of hospitalization, immature infants need parenteral nutrition to meet their nutritional requirements. Afterwards, nutrition is supplied via the enteral route using either enriched breast milk or preterm formula. However, replacing the nutrition provided by the placenta is difficult, and postnatal malnutrition and growth failure are commonly seen in preterm infants.
The brain is particularly vulnerable to the influences of nutrition between 24 and 42 weeks of gestation [2]. Thus, fetal and neonatal malnutrition may have global or isolated effects on the developing brain, depending on the requirements of the particular nutrients at the time of the deficit [2]. Both early and enhanced supply of energy, protein and lipids have shown to be beneficial for growth and neurodevelopment [3, 4]. Moreover, optimized nutrition has been shown to mediate disease severity [5].
The main target for feeding preterm infants is to achieve growth that resembles normal fetal growth rates [6] . In recent recommendations, this goal has been extended to achieving satisfactory functional development. The estimated amounts of nutrients necessary for growth similar to that of the fetal model are based on estimates obtained by factorial as well as empirical methods [6].
It is important to consider long-chain polyunsaturated fatty acids (LCPUFAs) due to their specific roles during the perinatal period. Therefore, the aim of this paper is to review the possible effects of LCPUFAs, particularly docosahexaenoic acid (DHA), on various clinical outcomes of preterm infants.
LCPUFA Metabolism during the Perinatal Period
The PUFAs linoleic acid and α-linolenic acid are essential fatty acids that must be provided exogenously [6, 7]. Linoleic acid is converted to arachidonic acid (AA) and α-linolenic acid to docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). Particularly AA and DHA accumulate rapidly during the last trimester and the first postnatal months, i.e. the period of rapid growth and brain development [6, 7]. DHA is the main lipid of the central nervous system and comprises as much as 30–50% of neuronal plasma membranes by weight [7, 8]. However, fetal brain accretion amounted to only 1.1 and 4.65% of the total body accretion of the omega-6 (n-6) and omega-3 (n-3) fatty acids, respectively [9]. Since most LCPUFAs accumulate in the white adipose tissue and to a lesser extent in the lean mass and in the liver, the DHA accumulation in other organs as well as the accumulation of other LCPUFAs is important to take into account when determining requirements.
AA and DHA are transferred by special transport molecules across the placenta to the fetus. The placenta provides the fetus with a selectivity which favors the transfer of DHA over all other fatty acids including AA [10]. There is evidence from stable isotope studies that AA and DHA synthesis can occur in premature infants. It has also been deduced from these tracer studies that the rate of AA synthesis is significantly greater than that of DHA, suggesting that the fetus has a greater ability to regulate its own levels of AA, not those of DHA, by de novo synthesis or reuptake by the placenta [10]. Overall, these data suggest that DHA supply may be more critical than that of AA during the perinatal period.
Studies conducted by using the LCPUFA precursors labeled with stable isotopes indicate that LCPUFA synthesis occurs even in small preterm infants and appears to be higher than in term infants. However, based on estimates of LCPUFA endogenous synthesis rates, premature infants appear to have an endogenous capacity for conversion of α-linolenic acid to DHA and EPA that cannot fulfill the requirement based on the fetal accretion rate [8, 11]. Furthermore, extremely premature infants are at increased risk of developing deficits in n-3 LCPUFAs due to the lack of adipose stores and limited provision of preformed LCPUFAs through nutritional sources.
The in utero accretion rate of DHA is estimated to be 43 and 212 mg/kg/day for DHA and AA, respectively [12]. It has been shown that current nutritional management of preterm infants leads to an early and severe DHA deficit, increasing with decreasing GA [13]. Depletion of DHA may lead to reduced visual function and alterations in behavior or cognitive performance [14], whereas DHA and AA supplementation has shown positive effects on growth, visual function and mental development in randomized controlled trials (RCT) [15–18].
Vision and Brain Development
In experimental studies, poor accumulation of retinal and brain DHA leads to abnormal retinal physiology, poor visual acuity, increased duration of visual fixation, and increased stereotyped behaviors and locomotor activity [14]. The evidence most relevant to the issue of causality showed that control performance levels can be restored when DHA is added to the diets of animals in which brain DHA concentration had been severely reduced. Nevertheless, the magnitude of these effects is not large, despite the fact that the studies were conducted under profound dietary restriction.
Studies in preterm infants indicate possible benefits for retinal and cognitive development, as suggested by greater retinal sensitivity to photic stimulation assessed by electroretinography, more mature visual acuity, and short-term effects on global developmental outcomes at 6–18 months after DHA supplementation of preterm infant formula in controlled clinical studies [19, 20].
With regard to neurodevelopment in preterm infants, recent meta-analyses suggest that benefits of formula supplementation with LCPUFA are less clear [21]. Among many possible explanations for the difficulty in demonstrating clinical benefits of LCPUFA supplementation in preterm formulas by meta-analysis are the extreme variability in study designs and the selection of relatively mature and healthy preterm infants which are likely less DHA deficient than very preterm infants. Furthermore, the meta-analyses include studies comparing some LCPUFA supplementation versus no supplementation and do not include studies comparing two doses of LCPUFAs. Interestingly, the amount of LCPUFAs used in early studies was chosen to produce the same concentration of AA and DHA in formula as in term breast milk (i.e. 0.2–0.4% fatty acids). This may not be a wise approach for preterm infants and, particularly, for very and extremely preterm infants because the amount of DHA provided by ingesting breast milk is below the in utero accretion rate [13].
Three studies report outcome data in preterm infants fed milk with a higher DHA content of 0.5–1.7% of total fatty acids. The first study, which examined the effect of providing DHA supplementation (0.50% of total fatty acids) for up to 9 months after term, showed that DHA improved growth in the whole cohort of preterm infants and improved mental development in boys [22]. In the second study, the effect of the supplementation during hospitalization of human milk with oils that provided an extra 32 mg of DHA and AA per 100 ml was assessed [15]. At the 6-month follow-up evaluation, the intervention group performed better than the control group in the problem-solving subscore of the Ages and Stages Questionnaire, and in the electrophysiologic assessment of event-related potentials, suggesting better recognition memory. At 20 months’ postnatal age, no differences in the mental and motor development scores of the Ages and Stages Questionnaire or in the Mental Development Index (MDI) score of the Bayley Scales of Infant Development were observed, but the intervention group had better results at 20 months at the free-play sessions, suggesting positive effects from supplementation on functions related to attention. Finally, plasma DHA concentration at discharge was positively correlated with the Bayley MDI and with ‘sustained attention’ [18]. Longterm follow-up, at 8 years of age, showed no effects on white matter microstructure, behavioral outcome, and cognitive functions [23, 24]. The third study was designed to compare the effects of a high versus standard DHA intake during hospitalization (i.e. 1 vs. 0.35% total fatty acids as DHA) while AA intake was kept constant (0.5% total fatty acids) [17, 25]. Visual acuity was improved significantly at 4 months corrected age. At 18 months, there were no overall differences in MDI or in the Psychomotor Developmental Index of the Bayley Scales, but fewer infants were classified as having an MDI score of less than 70. Infants who weighed <1,250 g and were fed the high-DHA diet had a higher MDI score than controls (mean difference = 4.6, 95% CI 0.1–9.0, p < 0.05), but the difference was not significant when GA at delivery, sex, maternal education, and birth order were taken into account. Girls, but not boys, fed a high-DHA diet had higher MDI scores and were less likely to have mild or significant developmental delay than control girls. Finally, the early advantage seen on visual and cognitive functions did not translate into any clinically meaningful change in visual and neurodevelopmental outcomes or behavior when assessed in childhood [26–28].
Studies show that providing larger amounts of DHA supplements is associated with better neurological outcomes at 18 months to 2 years
Overall, these studies show that providing larger amounts of DHA supplements is associated with better neurological outcomes at 18 months to 2 years (fig. 1). One study suggested that the smallest babies are the most vulnerable to DHA deficiency and likely to reap the greatest benefit from high-dose DHA supplementation. The observation that a nonsignificant difference in mean MDI translated to fewer infants with a low MDI score suggests that a high dose of DHA is more efficient, or is only efficient, in certain subgroups of infants, probably those at high risk of DHA deficiency.
Fig. 1. MDI (a) and Psychomotor Development Index (PDI) (b) scores of the Bayley Scales of Infant Development assessed at 18–20 months in preterm infants fed various amounts of DHA during hospitalization. Each dot represents one study group from references [17, 18, 22, 63, 64]. The amount of DHA is expressed as % of total fatty acids of either the mother’s milk or the formula fed during hospitalization.
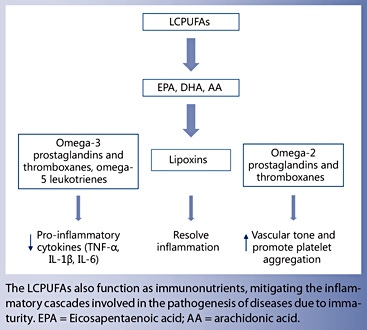
LCPUFAs as Immunonutrients
Immature infants are at risk of experiencing concomitant diseases due to immaturity, among these: bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), necrotizing enterocolitis (NEC), white matter injury of the brain (WMI), persistent ductus arteriosus, and septicemia. Perinatal infections or inflammation processes seem important in the pathogenesis of several of these comorbidities [29, 30]. Recent studies have demonstrated that immature infants have elevated levels of inflammatory cytokines during the neonatal period, and that upregulated cytokine expression is positively associated with BPD, ROP, WMI, and impaired neurodevelopmental outcomes [30–32] . A proposed mechanism behind the upregulated immune response is sustained activation (ongoing exogenous exposures) and/or impaired resolution of inflammation [31].
There is growing evidence that in addition to structural effects on growth and organ development, n-3 LCPUFAs, particularly DHA and EPA, may reduce the incidence or severity of BPD, ROP, NEC, and WMI by affecting different steps of the immune response [33, 34]. LCPUFAs have the capacity to influence the immune response by several means.
Certain LCPUFAs serve as precursors for the synthesis of eicosanoids (e.g. dihomo-γ-linolenic acid (20: 3n-6), AA, and EPA) and docosanoids (e.g. DHA). AA is a precursor of pro-inflammatory mediators (such as leukotrienes of the n-4 series), and of prostaglandins and thromboxanes of the n-2 series, which increase the vascular tone and promote platelet aggregation. AA is also a precursor of lipoxins which are inflammation-resolving mediators. In contrast, prostaglandins and thromboxanes of the n-3 series and leukotrienes of the n-5 series, formed from EPA, have many antagonistic effects such as a reduction in platelet aggregation and vascular tone as well as less inflammatory effects. Metabolites from EPA can modulate inflammation by decreasing the production of proinflammatory cytokines (TNF-α, IL-1β, and IL-6) through the peroxisome proliferator-activated receptor pathways, which in turn inhibits the nuclear transcription factor κB (NF-κB), and increasing the production and secretion of anti-inflammatory eicosanoids as interleukin-10 [33]. Resolvins, protectins, and maresins formed from n-3 LCPUFAs evoke anti-inflammatory and pro-resolving mechanisms, and enhance microbial clearance [34].
Bronchopulmonary Dysplasia
BPD is defined as persistent oxygen dependency at 36 weeks’ postmenstrual age and is, along with postnatal growth restriction, the most common morbidity of prematurity. BPD occurs mostly in infants born before 28 weeks of gestation [1]. BPD is characterized by diffuse fibrosis of the lung and impaired alveolar development [35]. Although the pathogenesis is multifactorial, intrauterine and postnatal growth restriction is an independent risk factor, possibly by affecting pulmonary alveolar and vessel growth [35].
Lipids have been considered toxic in acute respiratory failure since they may induce or intensify gas exchange abnormalities. The historical pure soybean lipid emulsion induces an increase in intrapulmonary shunt with reduction of the PaO 2 /FiO 2 ratio concordant with an increase in pulmonary blood pressure and vascular resistances [36]. In contrast there is some evidence from experimental studies that n-3 LCPUFAs may be beneficial in conditions associated with pulmonary hypertension through production of epoxides [37]. This, in turn, may reduce the need for mechanical ventilation and the risk of BPD.
The beneficial effect of DHA on lung function is supported by animal studies. For example, in a rat model of hyperoxia-induced lung injury, DHA supplementation was shown to decrease leukocyte infiltration in the pups of DHA supplemented nursing dams [38]. Separate studies have also demonstrated that exposure to high DHA increases the production of dipalmitoylphosphatidylcholine, the major surfactant lipid in the fetal and neonatal lung [39]. Some studies suggest that the use of a fish oil lipid emulsion or of a fish oil mixed lipid emulsion may reduce the risk of BPD and that adequate n-3 LCPUFA status may protect newborns from lung injuries induced by hyperoxia [40]. Along with sufficient early supply of protein and energy to promote growth, n-3 PUFAs seem to protect against lung injury or reduce BPD severity by a DHA-dependent activation of the peroxisome proliferator- activated receptor pathways, thereby accelerating lung maturation, pneumocyte growth and vasoproliferation [41].
In severe sepsis and in patients with acute lung injury, fatty acids from fish oil were found to attenuate the initial injurious hyperinflammatory state [42]. The bronchoalveolar lavages of adult patients with acute respiratory distress syndrome receiving n-3 fatty acids and γ-linoleic acid show an important decrease in global cell count, in polymorphonuclear cell percentage, IL-8 and leukotriene B 4 concentrations. The specific change in immune response was associated with an improvement of the PaO 2 / FiO 2 ratio, a reduction in mechanical ventilation need and duration, a decrease risk of complications, and a decreased length of stay in the intensive care unit [43].
Studies in preterm infants suggest improved lung development and a reduced incidence of BPD with fish oil supplementation [35]. The best evidence of the effects of n-3 fatty acids on the prevention of BPD comes from a large randomized trial assessing the effects of 60 mg/kg/ day DHA compared with a standard dose of 20 mg/kg/ day DHA on neurodevelopmental outcome of 657 preterm infants [17]. The study was not designed to test BPD; however, in exploratory analyses in the subgroup of infants less than 29 weeks’ GA, there was a significant reduction in infants requiring supplemental oxygen at 36 weeks’ postmenstrual age (RR 0.76, 95% CI 0.58–1.00, p = 0.05).
A recent meta-analysis targeting the role of LCPUFA supplementation in preterm infants born before 33 weeks of gestation found potential protective effects of n-3 fatty acids on BPD [44]. The effects were found for all interventions (RR 0.88, 95% CI 0.74–1.05) and in the subgroup of RCT that exclusively supplemented with n-3 LCPUFA (RR 0.84, 95% CI 0.66–1.13).
Retinopathy of Prematurity
In the retina, DHA is especially enriched in rod photoreceptor outer segments and essential for their differentiation, survival, and signal transduction [45]. ROP is a disorder of vascular development of the retina and it is the main reason for visual impairment in extreme premature infants. As for the lung, both nutritional and inflammatory factors seem to be important mediators in disease progression. Dietary n-3 LCPUFA reduces pathologic retinal neovascularization in oxygen-induced retinopathy in mice [46]. Two studies, one observational and one not blinded, reported a reduction in the need for laser therapy for ROP in very premature infants using fish oil supplementation in the lipid emulsion [47, 48]. Another study of infants with a GA of 28–31 weeks reported less ROP in fish oil-supplemented infants but no difference in need for treatment of proliferative disease [49]. Two other randomized controlled studies did not show any beneficial of fish oil lipid emulsion on ROP [50, 51].
While many studies have focused on DHA and its importance for vision and cognitive development, few studies have addressed the role of AA during fetal and neonatal life and after preterm birth. Just like DHA, AA is an important component of cell membranes where a change in composition results in changed function [52]. AA is an important precursor of factors, which appear essential for angiogenesis and thereby may play a significant role in the pathogenicity of ROP [52].
White Matter Injury
The most common brain injuries in premature infants are intraventricular hemorrhage and periventricular leukomalacia; with severe brain injury being defined as the presence of either intraventricular hemorrhage grade ≥ 3 or cystic periventricular leukomalacia. Indeed, WMI is associated with poor nutritional status as well as inflammation [29]. n-3 LCPUFAs, particularly DHA, are essential nutrients in brain development. In addition to being an important building block, DHA is also a substrate for neuroprotectin D1, which inhibits the pro-inflammatory cytokine production in human glial cells. In the same line of evidence, some experimental studies have shown that providing DHA may prevent neonatal brain injury by inhibiting oxidative stress and apoptosis of neuron cells [53]. Since most extremely premature infants receive insufficient amounts of DHA during neonatal hospitalization, providing adequate amounts of essential fatty acids to extremely premature infants, including preformed DHA and EPA, from birth onward, may improve neurodevelopmental outcome by mediating brain inflammation.
Sepsis and Noninfectious Inflammation
Very preterm infants are susceptible to sepsis, possibly as a result of attenuated innate immune responses [31] . Interestingly, these infants also show signs of sustained systemic inflammation with elevated pro-inflammatory cytokines. Sepsis may be defined as ‘the host’s deleterious and nonresolving systemic inflammatory response to microbial infection’ [54]. The host response is similar to the activation triggered by noninfectious tissue injuries like trauma, burns and ischemic reperfusion events [30], making it difficult to distinguish them from another. The newly identified alarmin molecule High Mobility Group Box 1 (HMGB1), which has been recognized as an important mediator of sepsis [30], is also thought to play an important role in lung injury and the pathogenesis of BPD [55]. HMGB1, an activator of NF-κB, is released by necrotic, but not apoptotic cells, and sustains the inflammatory process after the resolution of the early stage of inflammation [55]. As mentioned, one of the anti-inflammatory potentials of n-3 LCPUFAs is the ability to inhibit the activation of NF-κB [33], and thereby possibly modulate an inappropriate inflammatory response. These pathophysiological observations are in accordance with the observed association between low DHA and AA concentrations and the increased incidence of sepsis in preterm infants [58].
Necrotizing Enterocolitis
NEC is a serious disease of the gastrointestinal tract in very preterm infants and may lead to intestinal failure or death. The pathogenesis is multifactorial, but as with the other above-mentioned neonatal comorbidities, numerous inflammatory mediators seem to play a role in disease progression, among them HGMB1 [56, 57]. Several experimental models of NEC have demonstrated LCPUFA modulated reduction in both incidence and severity of bowel disease through multiple pathways associated with intestinal inflammation and necrosis [58–61]. The protective effects of DHA are multifactorial. Local cell membrane phospholipids play a structural role in protecting the integrity of intestinal cells and alterations in LCPUFA content is important in bacterial translocation and intracellular fluid shifts associated with cell stress signaling that initiates NEC [58].
Despite promising animal studies, results in preterm infants are mixed. In part, this may also be due to limited sample sizes, variable timing and dosing of DHA supplementation and similar confounding as described above. In an RCT, premature infants who were fed a DHA-supplemented formula had a decreased incidence of NEC compared to those who were fed a formula devoid of LCPUFAs [62]. Recently, a systematic review of n-3 LCPUFAs for extremely preterm infants found a trend toward a reduction in the risk of NEC (RR 0.50, 95% CI 0.23–1.10) [44].
There is growing evidence that n-3 LCPUFAs, particularly DHA and EPA, may reduce the incidence or severity of the most common comorbidities of prematurity
Conclusions
Since DHA accumulates in the central nervous system during development, a lot of attention has initially focused on the effects of DHA on neurodevelopment. Experimental studies as well as recent clinical trials show that providing larger amounts of DHA than currently and routinely provided is associated with better neurological outcomes at 18 months to 2 years. This early advantage, however, does not seem to translate into detectable change in visual and neurodevelopmental outcomes or behavior when assessed in childhood. However, this does not mean that supplementing with adequate amounts of LCPUFA during the perinatal period is not necessary.
Beside the effects on somatic development, there is growing evidence that n-3 LCPUFAs, particularly DHA and EPA, may reduce the incidence or severity of the most common comorbidities of prematurity by affecting different steps of the immune and anti-inflammatory response. These findings are of major clinical relevance mainly because infants born preterm, especially the smallest ones, are at particularly high risk for a nutritional deficit in n-3 fatty acids, predisposing to adverse neonatal outcomes. Further studies are warranted to address these issues as well as to more precisely determine the LCPUFA requirement in order to favor the best possible outcomes of preterm infants.
Acknowledgements
The authors thank the ‘Association pour la Recherche et la Formation En Neonatologie (ARFEN)’ for providing technical assistance.
Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose and have no financial disclosure to declare.
The writing of this article was supported by Nestlé Nutrition Institute.
References
Ancel PY, Goffinet F, Kuhn P, et al: Survival and morbidity of preterm children born at 22 through 34 weeks’ gestation in France in 2011: results of the EPIPAGE-2 cohort study. JAMA Pediatr 2015; 169: 230–238.
Georgieff MK: Nutrition and the developing brain: nutrient priorities and measurement. Am J Clin Nutr 2007; 85: 614S–620S.
Franz AR, Pohlandt F, Bode H, Mihatsch WA, Sander S, Kron M, Steinmacher J: Intrauterine, early neonatal, and postdischarge growth and neurodevelopmental outcome at 5.4 years in extremely preterm infants after intensive neonatal nutritional support. Pediatrics 2009; 123:e101–e109.
dit Trolli SE, Kermorvant-Duchemin E, Huon C, Bremond-Gignac D, Lapillonne A: Early lipid supply and neurological development at one year in very low birth weight (VLBW) preterm infants. Early Hum Dev 2012; 88(suppl 1):S25–S29.
Ehrenkranz RA, Das A, Wrage LA, Poindexter BB, Higgins RD, Stoll BJ, Oh W: Early nutrition mediates the influence of severity of illness on extremely LBW infants. Pediatr Res 2011; 69: 522–529.
Agostoni C, Buonocore G, Carnielli VP, et al: Enteral nutrient supply for preterm infants: commentary from the European society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J Pediatr Gastroenterol Nutr 2010; 50: 85–91.
Georgieff MK, Innis SM: Controversial nutrients that potentially affect preterm neurodevelopment: essential fatty acids and iron. Pediatr Res 2005; 57: 99R–103R.
Lapillonne A, Groh-Wargo S, Gonzalez CH, Uauy R: Lipid needs of preterm infants: updated recommendations. J Pediatr 2013; 162: S37–S47.
Innis SM: Essential fatty acid transfer and fetal development. Placenta 2005; 26(suppl A): S70–S75.
Haggarty P: Effect of placental function on fatty acid requirements during pregnancy. Eur J Clin Nutr 2004; 58: 1559–1570.
Lapillonne A, Jensen CL: Reevaluation of the DHA requirement for the premature infant. Prostaglandins Leukot Essent Fatty Acids 2009; 81: 143–150.
Kuipers RS, Luxwolda MF, Offringa PJ, Boersma ER, Dijck-Brouwer DA, Muskiet FA: Fetal intrauterine whole body linoleic, arachidonic and docosahexaenoic acid contents and accretion rates. Prostaglandins Leukot Essent Fatty Acids 2012; 86: 13–20.
Lapillonne A, Eleni Dit Trolli S, Kermorvant- Duchemin E: Postnatal docosahexaenoic acid deficiency is an inevitable consequence of current recommendations and practice in preterm infants. Neonatology 2010; 98: 397–403.
McCann JC, Ames BN: Is docosahexaenoic acid, an n-3 long-chain polyunsaturated fatty acid, required for development of normal brain function? An overview of evidence from cognitive and behavioral tests in humans and animals. Am J Clin Nutr 2005; 82: 281–295.
Henriksen C, Haugholt K, Lindgren M, Aurvag AK, Ronnestad A, Gronn M, Solberg R, Moen A, Nakstad B, Berge RK, Smith L, Iversen PO, Drevon CA: Improved cognitive development among preterm infants attributable to early supplementation of human milk with docosahexaenoic acid and arachidonic acid. Pediatrics 2008; 121: 1137–1145.
Isaacs EB, Ross S, Kennedy K, Weaver LT, Lucas A, Fewtrell MS: 10-year cognition in preterms after random assignment to fatty acid supplementation in infancy. Pediatrics 2011; 128:e890–e898.
Makrides M, Gibson RA, McPhee AJ, Collins CT, Davis PG, Doyle LW, Simmer K, Colditz PB, Morris S, Smithers LG, Willson K, Ryan P: Neurodevelopmental outcomes of preterm infants fed high-dose docosahexaenoic acid: a randomized controlled trial. JAMA 2009; 301: 175–182.
Westerberg AC, Schei R, Henriksen C, Smith L, Veierod MB, Drevon CA, Iversen PO: Attention among very low birth weight infants following early supplementation with docosahexaenoic and arachidonic acid. Acta Paediatr 2011; 100: 47–52.
Molloy C, Doyle LW, Makrides M, Anderson PJ: Docosahexaenoic acid and visual functioning in preterm infants: a review. Neuropsychol Rev 2012; 22: 425–437.
Lapillonne A: Enteral and parenteral lipid requirements of preterm infants. World Rev Nutr Diet 2014; 110: 82–98.
Fewtrell MS, Abbott RA, Kennedy K, Singhal A, Morley R, Caine E, Jamieson C, Cockburn F, Lucas A: Randomized, double-blind trial of long-chain polyunsaturated fatty acid supplementation with fish oil and borage oil in preterm infants. J Pediatr 2004; 144: 471–479.
Almaas AN, Tamnes CK, Nakstad B, Henriksen C, Grydeland H, Walhovd KB, Fjell AM, Iversen PO, Drevon CA: Diffusion tensor imaging and behavior in premature infants at 8 years of age, a randomized controlled trial with long-chain polyunsaturated fatty acids. Early Hum Dev 2016; 95: 41–46.
Almaas AN, Tamnes CK, Nakstad B, Henriksen C, Walhovd KB, Fjell AM, Due-Tonnessen P, Drevon CA, Iversen PO: Longchain polyunsaturated fatty acids and cognition in VLBW infants at 8 years: an RCT. Pediatrics 2015; 135: 972–980.
Smithers LG, Gibson RA, McPhee A, Makrides M: Higher dose of docosahexaenoic acid in the neonatal period improves visual acuity of preterm infants: results of a randomized controlled trial. Am J Clin Nutr 2008; 88: 1049–1056.
Smithers LG, Collins CT, Simmonds LA, Gibson RA, McPhee A, Makrides M: Feeding preterm infants milk with a higher dose of docosahexaenoic acid than that used in current practice does not influence language or behavior in early childhood: a follow-up study of a randomized controlled trial. Am J Clin Nutr 2010; 91: 628–634.
Collins CT, Gibson RA, Anderson PJ, McPhee AJ, Sullivan TR, Gould JF, Ryan P, Doyle LW, Davis PG, McMichael JE, French NP, Colditz PB, Simmer K, Morris SA, Makrides M: Neurodevelopmental outcomes at 7 years’ corrected age in preterm infants who were fed high-dose docosahexaenoic acid to term equivalent: a followup of a randomised controlled trial. BMJ Open 2015; 5:e007314.
Molloy CS, Stokes S, Makrides M, Collins CT, Anderson PJ, Doyle LW: Long-term effect of high-dose supplementation with DHA on visual function at school age in children born at <33 weeks gestational age: results from a follow-up of a randomized controlled trial. Am J Clin Nutr 2016; 103: 268– 275.
Dammann O, Leviton A: Inflammation, brain damage and visual dysfunction in preterm infants. Semin Fetal Neonatal Med 2006; 11: 363–368.
Strunk T, Inder T, Wang X, Burgner D, Mallard C, Levy O: Infection-induced inflammation and cerebral injury in preterm infants. Lancet Infect Dis 2014; 14: 751–762.
Marchant EA, Kan B, Sharma AA, van Zanten A, Kollmann TR, Brant R, Lavoie PM: Attenuated innate immune defenses in very premature neonates during the neonatal period. Pediatr Res 2015; 78: 492–497.
Paananen R, Husa AK, Vuolteenaho R, Herva R, Kaukola T, Hallman M: Blood cytokines during the perinatal period in very preterm infants: relationship of inflammatory response and bronchopulmonary dysplasia. J Pediatr 2009; 154: 39–43.e33.
Waitzberg DL, Torrinhas RS: Fish oil lipid emulsions and immune response: what clinicians need to know. Nutr Clin Pract 2009; 24: 487–499.
Serhan CN, Chiang N, Van Dyke TE: Resolving inflammation: Dual anti-inflammatory and pro-resolution lipid mediators. Nat Rev Immunol 2008; 8: 349–361.
Poindexter BB, Feng R, Schmidt B, Aschner JL, Ballard RA, Hamvas A, Reynolds AM, Shaw PA, Jobe AH: Comparisons and limitations of current definitions of bronchopulmonary dysplasia for the prematurity and respiratory outcomes program. Ann Am Thorac Soc 2015; 12: 1822–1830.
Hasselmann M, Reimund JM: Lipids in the nutritional support of the critically ill patients. Curr Opin Crit Care 2004; 10: 449– 455.
Houeijeh A, Aubry E, Coridon H, Montaigne K, Sfeir R, Deruelle P, Storme L: Effects of n-3 polyunsaturated fatty acids in the fetal pulmonary circulation. Crit Care Med 2011; 39: 1431–1438.
Rogers LK, Valentine CJ, Pennell M, Velten M, Britt RD, Dingess K, Zhao X, Welty SE, Tipple TE: Maternal DHA supplementation decreases lung inflammation in hyperoxia-exposed newborn mice. J Nutr 2010; 141: 214–222.
Blanco P, Freedman S, Lopez M, Ollero M, Comen E, Laposata M, Alvarez J: Oral docosahexaenoic acid given to pregnant mice increases the amount of surfactant in lung and amniotic fluid in preterm fetuses. Am J Obstet Gynecol 2004; 190: 1369–1374.
Sharma D, Nkembi AS, Aubry E, Houeijeh A, Butruille L, Houfflin-Debarge V, Besson R, Deruelle P, Storme L: Maternal PUFA omega- 3 supplementation prevents neonatal lung injuries induced by hyperoxia in newborn rats. Int J Mol Sci 2015; 16: 22081–22093.
Harris WS, Baack ML: Beyond building better brains: bridging the docosahexaenoic acid (DHA) gap of prematurity. J Perinatol 2015; 35: 1–7.
Singer P, Theilla M, Fisher H, Gibstein L, Grozovski E, Cohen J: Benefit of an enteral diet enriched with eicosapentaenoic acid and gamma-linolenic acid in ventilated patients with acute lung injury. Crit Care Med 2006; 34: 1033–1038.
Pacht ER, DeMichele SJ, Nelson JL, Hart J, Wennberg AK, Gadek JE: Enteral nutrition with eicosapentaenoic acid, gamma-linolenic acid, and antioxidants reduces alveolar inflammatory mediators and protein influx in patients with acute respiratory distress syndrome. Crit Care Med 2003; 31: 491–500.
Zhang P, Lavoie PM, Lacaze-Masmonteil T, Rhainds M, Marc I: Omega-3 long-chain polyunsaturated fatty acids for extremely preterm infants: a systematic review. Pediatrics 2014; 134: 120–134.
Politi L, Rotstein N, Carri N: Effects of docosahexaenoic acid on retinal development: cellular and molecular aspects. Lipids 2001; 36: 927–935.
Connor KM, SanGiovanni JP, Lofqvist C, Aderman CM, Chen J, Higuchi A, Hong S, Pravda EA, Majchrzak S, Carper D, Hellstrom A, Kang JX, Chew EY, Salem N Jr, Serhan CN, Smith LE: Increased dietary intake of omega-3-polyunsaturated fatty acids reduces pathological retinal angiogenesis. Nat Med 2007; 13: 868–873.
Pawlik D, Lauterbach R, Turyk E: Fish-oil fat emulsion supplementation may reduce the risk of severe retinopathy in VLBW infants. Pediatrics 2011; 127: 223–228.
Pawlik D, Lauterbach R, Walczak M, Hurkala J, Sherman MP: Fish-oil fat emulsion supplementation reduces the risk of retinopathy in very low birth weight infants: a prospective, randomized study. JPEN J Parenter Enteral Nutr 2014; 38: 711-716.
Beken S, Dilli D, Fettah ND, Kabatas EU, Zenciroglu A, Okumus N: The influence of fish-oil lipid emulsions on retinopathy of prematurity in very low birth weight infants: a randomized controlled trial. Early Hum Dev 2014; 90: 27–31.
D’Ascenzo R, Savini S, Biagetti C, Bellagamba MP, Marchionni P, Pompilio A, Cogo PE, Carnielli VP: Higher docosahexaenoic acid, lower arachidonic acid and reduced lipid tolerance with high doses of a lipid emulsion containing 15% fish oil: a randomized clinical trial. Clin Nutr 2014; 33: 1002–1009.
Vlaardingerbroek H, Vermeulen MJ, Carnielli VP, Vaz FM, van den Akker CH, van Goudoever JB: Growth and fatty acid profiles of VLBW infants receiving a multicomponent lipid emulsion from birth. J Pediatr Gastroenterol Nutr 2014; 58: 417–427.
Hadley KB, Ryan AS, Forsyth S, Gautier S, Salem N: The essentiality of arachidonic acid in infant development. Nutrients 2016; 8: pii:E216.
Suganuma H, Arai Y, Kitamura Y, Hayashi M, Okumura A, Shimizu T: Maternal docosahexaenoic acid-enriched diet prevents neonatal brain injury. Neuropathology 2010; 30: 597–605.
Vincent JL, Opal SM, Marshall JC, Tracey KJ: Sepsis definitions: time for change. Lancet 2013; 381: 774–775.
Aghai ZH, Saslow JG, Meniru C, Porter C, Eydelman R, Bhat V, Stahl G, Sannoh S, Pyon K, Hewitt C, Bhandari V: High-mobility group box-1 protein in tracheal aspirates from premature infants: relationship with bronchopulmonary dysplasia and steroid therapy. J Perinatol 2010; 30: 610–615.
Zamora R, Grishin A, Wong C, Boyle P, Wang J, Hackam D, Upperman JS, Tracey KJ, Ford HR: High-mobility group box 1 protein is an inflammatory mediator in necrotizing enterocolitis: protective effect of the macrophage deactivator semapimod. Am J Physiol Gastrointest Liver Physiol 2005; 289:G643– G652.
Lin PW, Stoll BJ: Necrotising enterocolitis. Lancet 2006; 368: 1271–1283.
Caplan MS, Russell T, Xiao Y, Amer M, Kaup S, Jilling T: Effect of polyunsaturated fatty acid (PUFA) supplementation on intestinal inflammation and necrotizing enterocolitis (NEC) in a neonatal rat model. Pediatr Res 2001; 49: 647–652.
Ohtsuka Y, Okada K, Yamakawa Y, Ikuse T, Baba Y, Inage E, Fujii T, Izumi H, Oshida K, Nagata S, Yamashiro Y, Shimizu T: Omega-3 fatty acids attenuate mucosal inflammation in premature rat pups. J Pediatr Surg 2011; 46: 489–495.
Lu J, Jilling T, Li D, Caplan MS: Polyunsaturated fatty acid supplementation alters proinflammatory gene expression and reduces the incidence of necrotizing enterocolitis in a neonatal rat model. Pediatr Res 2007; 61: 427–432.
De Plaen IG, Liu SX, Tian R, Neequaye I, May MJ, Han XB, Hsueh W, Jilling T, Lu J, Caplan MS: Inhibition of nuclear factor-κB ameliorates bowel injury and prolongs survival in a neonatal rat model of necrotizing enterocolitis. Pediatr Res 2007; 61: 716–721.
Carlson SE, Montalto MB, Ponder DL, Werkman SH, Korones SB: Lower incidence of necrotizing enterocolitis in infants fed a preterm formula with egg phospholipids. Pediatr Res 1998; 44: 491–498.
Fewtrell MS, Morley R, Abbott RA, Singhal A, Isaacs EB, Stephenson T, MacFadyen U, Lucas A: Double-blind, randomized trial of long-chain polyunsaturated fatty acid supplementation in formula fed to preterm infants. Pediatrics 2002; 110: 73–82.
Clandinin MT, Van Aerde JE, Merkel KL, Harris CL, Springer MA, Hansen JW, Diersen- Schade DA: Growth and development of preterm infants fed infant formulas containing docosahexaenoic acid and arachidonic acid. J Pediatr 2005; 146: 461–468.