Docosahexaenoic Acid and Neurodevelopmental Outcomes of Term Infants
29 min read
/
Key insights
Although there is ample evidence highlighting the importance of docosahexaenoic acid (DHA) in the development and function of the central nervous system (CNS), clinical data on the effects of dietary DHA on neurocognitive outcomes remains inconclusive. Despite the existence of clear dietary intake recommendations for pregnant and lactating women, DHA levels are insufficient even across the populations of many developed countries.
Current knowledge
DHA and arachidonic acid are long-chain polyunsaturated fatty acids (LCPUFA) essential for development and overall health. High concentrations of DHA are found within the lipid bilayer of neurons, affecting membrane fluidity and neuronal transmission. DHA also modulates the function of other membrane-bound proteins, such as enzymes, ion channels and receptors. Deposition of DHA in the brain peaks during the third trimester of pregnancy and during the first year of life, coinciding with the period of rapid brain growth. During fetal development, circulating maternal DHA is sequestered by the growing fetus. The DHA requirements of infants are met through the diet, either from breast milk or formula.
Practical implications
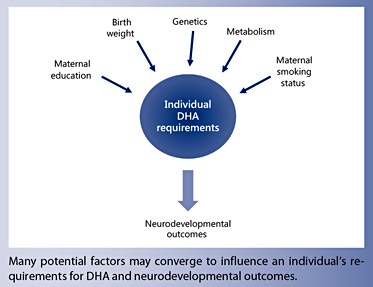
Despite the positive findings from some observational studies, many randomized controlled intervention trials have failed to demonstrate a conclusive benefit of maternal DHA supplementation on infant neurodevelopment. Few trials have evaluated supplementation during the lactation period. In contrast, many trials have been conducted on LCPUFA supplementation of infant formula. Regardless of the time period of the intervention, there is a large degree of heterogeneity between the studies with respect to the DHA dose, the intervention period and outcomes assessed. These trials do not demonstrate a benefit of DHA supplementation of healthy infants on child development. The individual response to prenatal DHA levels may be influenced by other factors, such as genetic background, smoking, maternal education and birth weight. This suggests that future efforts should focus on characterizing the responders to DHA to clarify the role of optimal dose and timing of potential interventions.
Recommended reading
Hibbeln JR, Davis JM, Steer C, et al: Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet 2007;369:578–585.
Supplementation with docosahexaenoic acid (DHA) or fish oil during pregnancy and/or lactation does not improve child development.
Supplementation of healthy infants with DHA or fish oil does not improve child development.
Key Words
Docosahexaenoic acid · Long-chain polyunsaturated fatty acid · Fish oil · Child development
Abstract
Docosahexaenoic acid (DHA), a long-chain polyunsaturated fatty acid, is essential for normal brain development. DHA is found predominantly in seafood, fish oil, breastmilk and supplemented formula. DHA intake in Western countries is often below recommendations. Observational studies have demonstrated an association between DHA intake in pregnancy and neurodevelopment of offspring but cannot fully adjust for confounding factors that influence child development. Randomised clinical trials of DHA supplementation during pregnancy and/or lactation, and of term infants, have not shown a consistent benefit nor harm on neurodevelopment of healthy children born at term. The evidence does not support DHA supplementation of healthy pregnant and lactating women, nor healthy infants.
The Role of Docosahexaenoic Acid in the Neurodevelopment of the Fetus and Infant
Long-chain polyunsaturated fatty acids (LCPUFA), including docosahexaenoic acid (DHA) and arachidonic acid are essential for overall health including normal growth, vision and, specific to this review, neurodevelopment. Peak brain deposition of DHA occurs during the third trimester of gestation and during the first year, coinciding with rapid brain growth [1]. Infants are provided with DHA during early development of the central nervous system (CNS) predominantly through placental transfer during gestation and through dietary intake postnatally [2]. Despite intake recommendations for pregnant and lactating women existing between 200–300 mg per day [3, 4], intake in Western nations may be insufficient due to the high demands of the fetus and inadequate maternal intake [5]. Postnatally, while breast milk and/or infant formula may contain DHA, the amount provided will vary based on maternal dietary intake and brand of formula, respectively. Countries that typically experience low levels of DHA within breast milk are Western nations such as the USA (0.2%), Canada (0.14%) and Australia (0.25%) [6].
There have been a number of expert reviews detailing the evidence for the roles of DHA during early CNS development [7–11], and each highlights the importance of DHA for optimal function. DHA is found at high concentrations within the lipid bilayer of neurons, playing a functional role in fluidity/flexibility of the membrane affecting neuronal transmission [12]. Furthermore, evidence suggests that DHA also has demonstrable effects upon the activities of membrane-bound enzymes, ion channels and receptors, gene expression and neuronal inflammation via eicosanoid precursors [13]. Specific to neurodevelopment, the high proportion of DHA in neural membranes suggests that DHA is important for membrane biogenesis and, consequently, such events as neurogenesis, neuronal migration and outgrowth [7, 8].
The importance of DHA during CNS development has led to the hypothesis that early diet modulation of DHA may alter the normal trajectory of brain development, and subsequently affect the functional skills derived from CNS structures. Research has been undertaken investigating how and in what quantities DHA is supplied to the infant CNS, and whether such quantities are sufficient to support optimal brain function.
Associations between DHA Intake (Maternal and Neonatal/Infant) and Neurodevelopment of the Fetus and Infant
Observational trials provide data showing that maternal and infant omega-3 (n-3) LCPUFA consumption and/or status may positively influence infant neurodevelopment. Significant positive associations have been reported for specific outcomes in a number of maternal studies [14–22] , with a smaller number observing negative associations [18, 20, 22, 23] , or no associations [21– 25] . Benefits for a wide range of outcomes have been found such as verbal intelligence quotient, language, motor and neurological development and social behaviour. Despite some consistency of results, study methodology is variable, particularly for the sample size, the measurement of DHA via food frequency questionnaire or specific cell fractions and the impact of confounding factors including socioeconomic status.
The largest study to date was conducted by Hibbeln et al. [17] in 2007, whereby seafood consumption <340 g/ week at 32 weeks’ gestation was associated with an increased risk of lowest-quartile verbal intelligence in the offspring at 8 years. The strength of this study lies in the large sample size of 11,875 participants, far greater than the majority of other trials. The study concluded that pregnant women should not reduce seafood consumption during pregnancy, and by doing so may lose benefits to offspring neurodevelopment.
A recent study of this design was conducted by Julvez et al. [26]. In a population characterised by high seafood consumption (Spain), moderate positive associations were found between seafood consumption during the first and third trimesters of pregnancy and child neuropsychological development at 5 years. Yet, following adjustment for cord-blood LCPUFA levels, only part of the significance remained, suggesting that the beneficial effect was not only derived from DHA consumption. Herein lies the difficulty in the interpretation of such trials. Such observational studies are unable to establish causality because of the difficulty in adjusting for the complex confounding factors that also influence early child development.
Observational studies are unable to establish causality because of the difficulty in adjusting for the complex confounding factors that also influence early child development
To explore this, Gould et al. [27] recently conducted an association study to explore what maternal factors influenced DHA status during pregnancy. Their results suggested that responsiveness to prenatal DHA was related to the characteristics of the specific population groups studied. In the Australian cohort examined by the authors, birth weight, maternal education and smoking were seen to interact with DHA status during pregnancy and neurodevelopment. Such findings suggest that either future trials power their studies sufficiently to be able to evaluate subgroup analyses post hoc, or that responders to DHA supplementation are identified prior to supplementation. Either way will require significant changes to the design or sample sizes of future observational trials.
For infant and childhood association studies, results are more mixed, with studies showing a combination of Observational studies are unable to establish causality because of the difficulty in adjusting for the complex confounding factors that also influence early child development DHA and Neurodevelopmental Outcomes of Term Infants Ann Nutr Metab 2016;69(suppl 1):23–28 DOI: 10.1159/000448271 25 negative or no association [18, 28, 29], compared to positive [16, 30, 31]. This may highlight the importance of the maternal period for DHA accretion.
Randomised Controlled Trials of Maternal LCPUFA Supplementation and Infant Neurodevelopment
A number of randomised controlled trials (RCTs) have been undertaken to ascertain if maternal LCPUFA supplementation is an effective strategy for improving offspring neurodevelopment. A recent meta-analysis conducted by Gould et al. [32] included 11 RCTs totalling 5,272 participants and observed no significant differences between the supplemented groups for cognitive, language or motor development. A single finding for enhanced cognitive scores for children aged 2.5 years was detected; yet, this effect was ascertained from 2 trials with a high risk of bias and the authors advised caution in interpretation. The methodological quality of the trial was generally observed as poor, particularly the sample sizes, the high attrition rates and statistical design.
The largest maternal supplementation study to date was conducted by Makrides et al. [33] in 2010: 726 pregnant women were supplemented with 800 mg/day of either fish oil or placebo during the second half of pregnancy. The study had a high level of methodological rigour with low attrition. No effects of DHA treatment during pregnancy on neurodevelopment were identified, either at 18 months or in a more recent follow-up at 4 years. Further, in a subset of this cohort, 158 children were assessed at 27 months for attention, working memory and inhibitory control. No significant differences were observed between the groups, except with a small number of inconsistent effects which were attributed to chance.
Since 2013, two new RCTs have been published, both of which found no statistically significant effects of maternal DHA supplementation. Ramakrishnan et al. [34] recruited 730 women in Mexico supplemented daily with either 400 mg DHA or placebo capsules from 18–22 weeks’ gestation until delivery and found no effects on neurodevelopment at 18 months of age using the Bayley Scales of Infant Development (BSID) (Spanish version). Hurtado et al. [35] recruited 110 pregnant women to an RCT of 400 mg DHA per day from 28 weeks’ gestation until the end of lactation, assessing neurodevelopment at 12 months of age. No differences were observed between groups, also according to the BSID. However, attrition in the study was high and only ∼ 40% of the study participants were assessed for neurodevelopment.
Overall, results from maternal supplementation RCTs still appear inconclusive. Yet, it can be noted that controlled studies have not shown the same consistent positive findings that observational trials have yielded. While this may be a result of heterogeneity in study design, and in many cases insufficient methodological quality, it remains possible that supplementation with DHA during pregnancy may not confer any neurological benefit to the offspring. Particular difficulties in the design of maternal RCTs are identifying what dose should be administered, when neurodevelopmental testing should take place and what specific neurodevelopmental tests should be administered.
Particular difficulties in the design of maternal RCTs are identifying what dose should be administered, when neurodevelopmental testing should take place and what specific neurodevelopmental tests should be administered
RCTs of Supplementation during Lactation and Infant Neurodevelopment
The investigation of DHA supplementation during lactation for improved infant and child neurodevelopment has been less specifically examined in the recent literature. A number of maternal supplementation trials have continued to supplement mothers during lactation [36], but such a design makes it difficult to identify during which time period supplementation was beneficial. Overall, studies including both maternal and lactation supplementation with DHA have not observed any significant effects on neurodevelopment.
A Cochrane analysis conducted by Delgado-Noguera et al. [37] in 2010 reviewed RCTs of LCPUFA supplementation during lactation, and included 6 trials totalling 1,280 women. Supplementation trials of both pregnancy and lactation, along with lactation only, were included. No significant differences were observed as a result of supplementation for children’s neurodevelopment. Yet, following a sensitivity analysis, a significant benefit was observed for psychomotor development at 5 years based on only 1 trial [38] . The trials were ascribed as having a low risk of bias and an overall rigorous methodology, and the authors suggested that more trials were required for more conclusive findings to be reached.
Only three trials have investigated lactation specifically [38–40]. Similar to the trials of maternal supplementation, the optimal concentration of DHA within breast milk to confer any neurological benefit is as yet unknown. Breast milk DHA levels vary worldwide, with concentrations of as high as 1% noted in countries with high fish intake such as Japan [6]. Using five different doses of DHA supplementation for 12 weeks after birth, Gibson et al. [39], in 1997, observed little further increase in infant plasma or erythrocyte DHA levels when breast milk was above 0.8% of total fatty acids. In this study, higher mental development index scores using the Bayley scales were associated with higher breast milk DHA status at 12 months; yet, this effect was not observed at 2 years.
The optimal concentration of DHA within breast milk to confer any neurological benefit is as yet unknown
In a high-dose trial, Lauritzen et al. [40] in Denmark supplemented 122 mothers with low fish intake to fish oil or placebo supplementation for the first 4 months of lactation (800 mg DHA and 600 mg eicosapentaenoic acid). A third group of breastfeeding women with high fish intake were included as a reference. It was observed that vocabulary at 1 year was lower in the children of the fish oil-supplemented group compared to children in the control group, but this finding was not observed at 2 years. In contrast, in 2005, Jensen et al. [38] conducted a study supplementing breastfeeding mothers using DHA algal oil (approx. 200 mg DHA per day) for 4 months after delivery. Despite maternal DHA phospholipid contents increasing to 75% higher than baseline, neurodevelopment and vision were unaffected during the first 12 months. However, at 30 months of age, the supplemented group had a higher Bayley psychomotor development index (but not a higher mental development index). Again at 5 years of age, children whose mothers received DHA versus placebo performed significantly better on the sustained attention subscale of the Leiter International Performance Scale.
In summary, for trial of DHA supplementation during lactation, further trials are necessary in order to definitively conclude if supplementation can improve infant and child neurodevelopment. Sufficient statistical power, long-term follow-up and an investigation of optimal dosage are required.
DHA Supplementation of Term Infants (Formula and Direct Supplementation) and Neurodevelopment
RCTs of LCPUFA supplementation of infant formula have been conducted for the past 30 years and came about due to the lack of LCPUFA in commercial infant formulas compared to breast milk. While a relatively large number of trials have been conducted, there is a large degree of heterogeneity between studies, in particular regarding the dose of DHA, the length of supplementation and the method of assessment [41, 42]. Furthermore, the more recent identification of the genetic control of PUFA metabolism has raised the question of individual variability for DHA requirements. Two recent meta-analyses have been completed, one including 15 trials [43] and another evaluating 12 [44]. Both found no beneficial effects of supplementation on either mental or psychomotor development. Yet, Koletzko et al. [45], in a systematic review including 5 trials not evaluated by the previous metaanalyses, commented on the lack of consistency of RCTs, but noted a trend towards a greater likelihood of benefit with higher dosages ( ≥ 0.32% DHA and ≥ 0.66% arachidonic acid) and a longer duration of higher postnatal LCPUFA supplementation (up to 1 year of age).
Regarding the method of neurodevelopmental assessment, Sun et al. [42] lately assessed the validity and reliability of such measures used in LCPUFA supplementation trials. Using 29 articles, they noted that the methods of assessment all lacked predictive validity for future neurocognitive performance, and that measures of intellectual ability are usually not subject to change in the short term. They identified that a ‘well-designed, valid and clinical outcome assessment that measures neurocognitive function in neonates and infants is essential to provide the scientific evidence required for future clinical trials’. Yet, it was noted by the authors that no such measures exist, and therefore future collaboration and research towards such goals should be completed. Until this has taken place, determining the impact of DHA supplementation for infants may remain elusive.
Conclusions
There is no definite evidence that DHA supplementation in pregnancy, lactation or infancy improves the neurodevelopment of healthy term infants. If future trials are to provide certainty, they will need to recruit large sample sizes to identify potential subgroup analyses, such as maternal factors, infant gender and genetics, identify the optimal dose for supplementation and assess using well-designed and valid measures.
Disclosure Statement
The authors have no conflicts of interest to disclose.
The writing of this article was supported by Nestlé Nutrition Institute.
References
Martinez M: Tissue levels of polyunsaturated fatty acids during early human development. J Pediatr 1992; 120(4 Pt 2):S129–S138.
Innis SM: Essential fatty acid transfer and fetal development. Placenta 2005; 26(suppl A): S70–S75.
Simopoulos AP, Leaf A, Salem N Jr: Workshop on the essentiality of and recommended dietary intakes for omega-6 and omega-3 fatty acids. J Am Coll Nutr 1999; 18: 487–489.
Koletzko B, Cetin I, Brenna JT: Dietary fat intakes for pregnant and lactating women. Br J Nutr 2007; 98: 873–877.
Makrides M: Is there a dietary requirement for DHA in pregnancy? Prostaglandins Leukot Essent Fatty Acids 2009; 81: 171–174.
Brenna JT, et al: Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am J Clin Nutr 2007; 85: 1457–1464.
Lauritzen L, et al: DHA Effects in brain development and function. Nutrients 2016; 8: 6.
Lauritzen L, et al: The essentiality of long chain n-3 fatty acids in relation to development and function of the brain and retina. Prog Lipid Res 2001; 40: 1–94.
Heird WC, Lapillonne A: The role of essential fatty acids in development. Annu Rev Nutr 2005; 25: 549–571.
Neuringer M, Anderson GJ, Connor WE: The essentiality of n-3 fatty acids for the development and function of the retina and brain. Annu Rev Nutr 1988; 8: 517–541.
Hashimoto M, et al: The hypotensive effect of docosahexaenoic acid is associated with the enhanced release of ATP from the caudal artery of aged rats. J Nutr 1999; 129: 70–76.
Horrocks LA, Farooqui AA: Docosahexaenoic acid in the diet: its importance in maintenance and restoration of neural membrane function. Prostaglandins Leukot Essent Fatty Acids 2004; 70: 361–372.
Williams C, et al: Stereoacuity at age 3.5 years in children born full-term is associated with prenatal and postnatal dietary factors: a report from a population-based cohort study. Am J Clin Nutr 2001; 73: 316–322.
Oken E, et al: Maternal fish consumption, hair mercury, and infant cognition in a U.S. cohort. Environ Health Perspect 2005; 113: 1376–1380.
Daniels JL, et al: Fish intake during pregnancy and early cognitive development of offspring. Epidemiology 2004; 15: 394–402.
Hibbeln JR, et al: Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet 2007; 369: 578–585.
Mendez MA, et al: Maternal fish and other seafood intakes during pregnancy and child neurodevelopment at age 4 years. Public Health Nutr 2009; 12: 1702–1710.
Oken E, et al: Associations of maternal fish intake during pregnancy and breastfeeding duration with attainment of developmental milestones in early childhood: a study from the Danish National Birth Cohort. Am J Clin Nutr 2008; 88: 789–796.
Strain J, et al: Prenatal exposure to methyl mercury from fish consumption and polyunsaturated fatty acids: associations with child development at 20 mo of age in an observational study in the Republic of Seychelles. Am J Clin Nutr 2015; 101: 530–537.
Oken E, et al: Maternal fish intake during pregnancy, blood mercury levels, and child cognition at age 3 years in a US cohort. Am J Epidemiol 2008; 167: 1171–1181.
Gale CR, et al: Oily fish intake during pregnancy– association with lower hyperactivity but not with higher full-scale IQ in offspring. J Child Psychol Psychiatry 2008; 49: 1061– 1068.
Sagiv SK, et al: Prenatal exposure to mercury and fish consumption during pregnancy and attention-deficit/hyperactivity disorder-related behavior in children. Arch Pediatr Adolesc Med 2012; 166: 1123–1131.
Davidson PW, et al: Neurodevelopmental effects of maternal nutritional status and exposure to methylmercury from eating fish during pregnancy. Neurotoxicology 2008; 29: 767–775.
Suzuki K, et al: Neurobehavioral effects of prenatal exposure to methylmercury and PCBs, and seafood intake: neonatal behavioral assessment scale results of Tohoku study of child development. Environ Res 2010; 110: 699–704.
Julvez J, et al: Maternal consumption of seafood in pregnancy and child neuropsychological development: a longitudinal study based on a population with high consumption levels. Am J Epidemiol 2016; 183: 169– 182.
Gould JF, et al: Maternal characteristics influence response to DHA during pregnancy. Prostaglandins Leukot Essent Fatty Acids 2016; 108: 5–12.
Engel S, et al: Docosahexaenoic acid status at 9 months is inversely associated with communicative skills in 3-year-old girls. Matern Child Nutr 2013; 9: 499–510.
Fahmida U, et al: Genetic variants of FADS gene cluster, plasma LC-PUFA levels and the association with cognitive function of under- two-year-old Sasaknese Indonesian children. Asia Pac J Clin Nutr 2015; 24: 323– 328.
Theodore RF, et al: Dietary patterns and intelligence in early and middle childhood. Intelligence 2009; 37: 506–513.
Freire C, et al: Hair mercury levels, fish consumption, and cognitive development in preschool children from Granada, Spain. Environ Res 2010; 110: 96–104.
Gould JF, Smithers LG, Makrides M: The effect of maternal omega-3 (n − 3) LCPUFA supplementation during pregnancy on early childhood cognitive and visual development: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr 2013; 97: 531–544.
Makrides M, et al: Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: a randomized controlled trial. JAMA 2010; 304: 1675–1683.
Ramakrishnan U, et al: Prenatal docosahexaenoic acid supplementation and offspring development at 18 months: randomized controlled trial. PLoS One 2015; 10: e0120065.
Hurtado JA, et al: Effects of maternal Ω-3 supplementation on fatty acids and on visual and cognitive development. J Pediatr Gastroenterol Nutr 2015; 61: 472–480.
Helland IB, et al: Similar effects on infants of n-3 and n-6 fatty acids supplementation to pregnant and lactating women. Pediatrics 2001; 108:E82.
Delgado-Noguera MF, Calvache JA, Bonfill Cosp X: Supplementation with long chain polyunsaturated fatty acids (LCPUFA) to breastfeeding mothers for improving child growth and development. Cochrane Database Syst Rev 2010;(12):CD007901.
Jensen CL, et al: Effects of maternal docosahexaenoic acid intake on visual function and neurodevelopment in breastfed term infants. Am J Clin Nutr 2005; 82: 125–132.
Gibson RA, Neumann MA, Makrides M: Effect of increasing breast milk docosahexaenoic acid on plasma and erythrocyte phospholipid fatty acids and neural indices of exclusively breast fed infants. Eur J Clin Nutr 1997; 51: 578–584.
Lauritzen L, et al: Maternal fish oil supplementation in lactation: effect on developmental outcome in breast-fed infants. Reprod Nutr Dev 2005; 45: 535–547.
Meldrum SJ, et al: Achieving definitive results in long-chain polyunsaturated fatty acid supplementation trials of term infants: factors for consideration. Nutr Rev 2011; 69: 205–214.
Sun H, et al: Infant formula and neurocognitive outcomes: impact of study end-point selection. J Perinatol 2015; 35: 867–874.
Simmer K, Patole SK: Longchain polyunsaturated fatty acid supplementation in infants born at term. Cochrane Database Syst Rev 2008;(1):CD000376.
Qawasmi A, et al: Meta-analysis of longchain polyunsaturated fatty acid supplementation of formula and infant cognition. Pediatrics 2012; 129: 1141–1149.
Koletzko B, et al: The roles of long-chain polyunsaturated fatty acids in pregnancy, lactation and infancy: review of current knowledge and consensus recommendations. J Perinat Med 2008; 36: 5–14.