Infants receive large amounts of human milk oligosaccharides (HMOs) with a high potential for local effects within the gastrointestinal tract and for systemic functions. In feces and urine, native HMOs and degradation products are present which partly refl ect the mothers’ specifi c milk oligosaccharide pattern.
Introduction
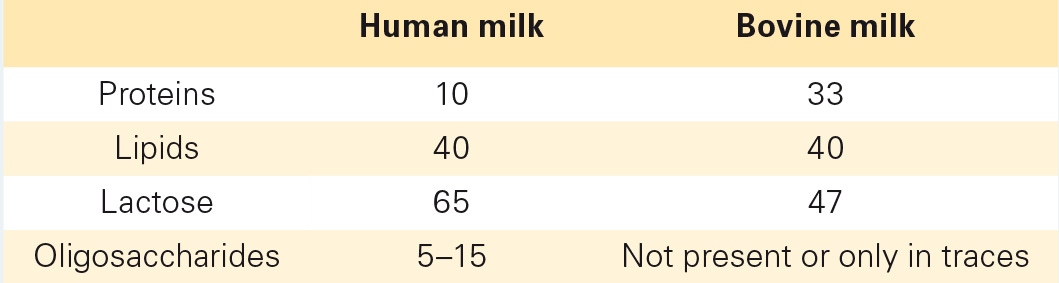
In recent years, there has been a tremendous increase in our knowledge regarding specifi c effects of human milk oligosaccharides (HMOs) which are not or only in trace amounts present in bovine milk (table 1). Concomitantly with these studies, progress in biotechnology nowadays allows to produce at least some HMOs to potentially be added to infant formulas. To decide which compound(s) would be most suitable for supplementation, in which concentrations or combinations, and how long it should be given, studies are needed regarding their metabolic fate as well as their local and systemic effects.
Table 1. Composition of major components in human and bovine milk (in g/l)
History
Important observations with regard to infants’ health have already been made around 1900. The discovery of lactobacilli and bifi dobacteria and their relevance for health and disease was an important milestone. At the same time, pediatricians realized that the fecal composition of breast-fed and bottle- fed infants differed. Observations indicated that this difference is particularly linked to the milk carbohydrate fraction. This was the starting point of research on human milk carbohydrates. In the following years, the fi rst HMOs were identifi ed [1]. Studies conducted after 1950 focused on the identifi cation of various HMOs as the ‘bifi - dus factor’ in human milk [2]. Since then, about 150 single HMOs have been characterized. It is important to note that the Lewis blood group and the secretor/non-secretor status lead to very specifi c HMO patterns in milk which are discussed of having an infl uence on certain diseases [3].
Structures
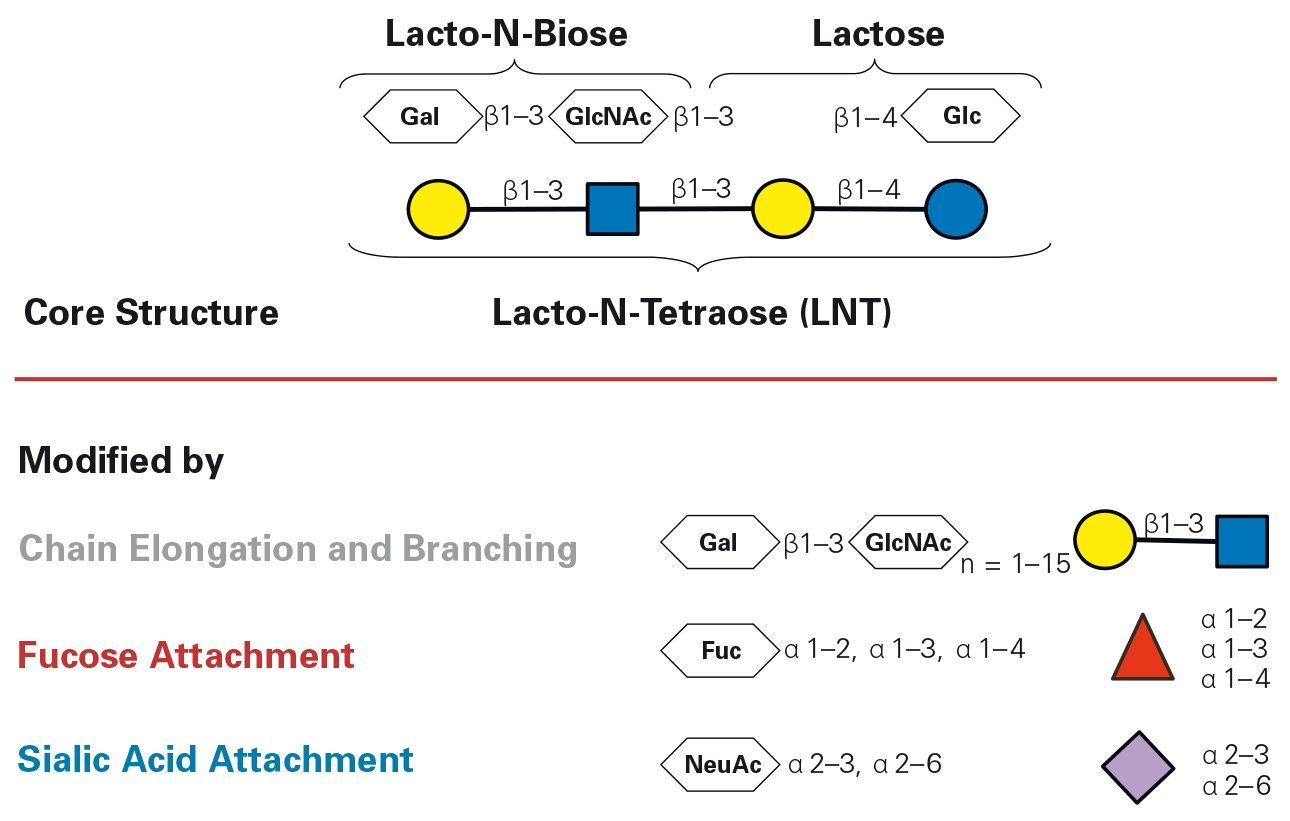
Almost all HMOs are based upon lactose which is modifi ed in the mammary gland by the attachment of monosaccharides such as fucose, N-acetylglucosamine, and/or sialic acid (fi g. 1). Thus, complex structures with very specifi c linkages are built, which is the basis for the multifunctionality of HMOs [3, 4].
Fig 1. Composition of HMOs and potential modifi cations.
Physiological Observations as Background to HMO Research
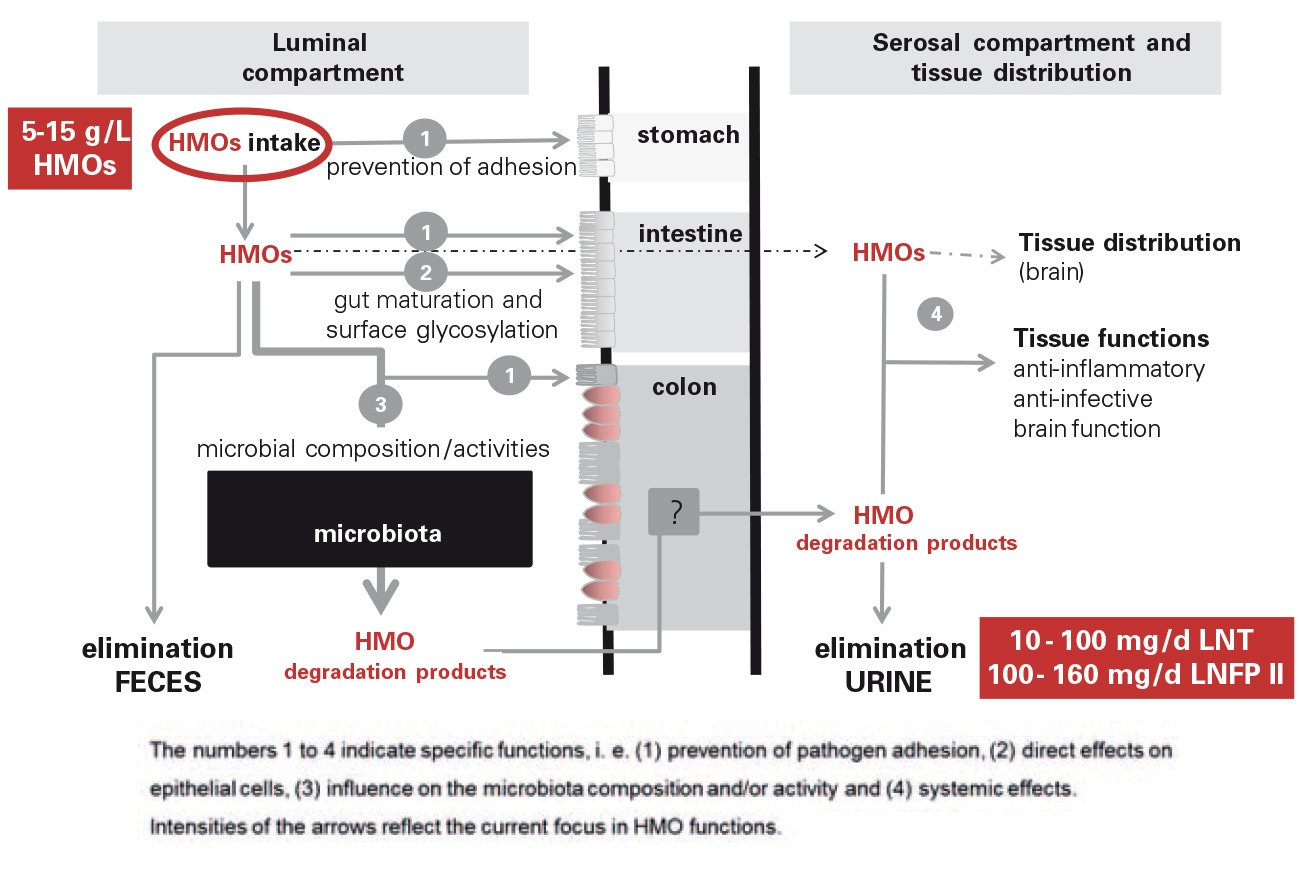
Large amounts of HMOs, i.e. several grams per day, rinse the gastrointestinal tract of a human milk-fed infant, thereby potentially preventing pathogen adhesion to the intestinal mucosa or infl uencing gut maturation processes [5, 6]. HMOs are considered not to be degraded by human digestive enzymes and transported into the lower parts of the intestine where they may be metabolized by the microbiota or get excreted with feces [7–10]. As about 1–2% of HMOs are excreted via the infants’ urine (fi g. 2), several hundred milligrams per day may circulate in the infants’ blood, which is enough to suppose systemic functions such as anti-infl ammatory or anti-infective effects of HMOs.
Fig. 2. Intake, metabolism, and potential functions of HMOs.
References
Kuhn R: Oligosaccharides of milk (in French). Bull Soc Chim Biol (Paris) 1958;40:297–314.
György P: A hitherto unrecognized biochemical difference between human milk and cow’s milk. J Pediatr 1953;11:98–108.
Kunz C, Kuntz S, Rudloff S: Bioactivity of human milk oligosaccharides; in Moreno FJ, Sanz ML (eds): Food Oligosaccharides: Production, Analysis and Bioactivity. Oxford, Wiley-Blackwell, 2014, pp 5–17.
Bode L, Jantscher-Krenn E: Structure-function relationships of human milk oligosaccharides. Adv Nutr 2012;3:383S–391S.
Rudloff S, Kunz C: Milk oligosaccharides and metabolism in infants. Adv Nutr 2012;3:398S–405S.
Rudloff S, Pohlentz G, Borsch C, Lentze MJ, Kunz C: Urinary excretion of in vivo 13C-labelled milk oligosaccharides in breastfed infants. Br J Nutr 2012;107: 957–963.
Dotz V, Rudloff S, Meyer C, Lochnit G, Kunz C: Metabolic fate of neutral human milk oligosaccharides in exclusively breast-fed infants. Mol Nutr Food Res 2015;59: 355–364.
Asakuma S, Hatakeyama E, Urashima T, Yoshida E, Katayama T, Yamamoto K, Kumagai H, Ashida H, Hirose J, Kitaoka M: Physiology of consumption of human milk oligosaccharides by infant gut-associated bifi dobacteria. J Biol Chem 2011;286:34583– 34592.
Sela DA, Mills DA: Nursing our microbiota: molecular linkages between bifi dobacteria and milk oligosaccharides. Trends Microbiol 2010;18:298–307.
Wang M, Li M, Wu S, Lebrilla CB, Chapkin RS, Ivanov I, Donovan SM: Fecal microbiota composition of breast-fed infants is correlated with human milk oligosaccharides consumed. J Pediatr Gastroenterol Nutr 2015;60:825–833.